
Obesity: Definitions and Differences
The worldwide prevalence of obesity is increasing and airway management in the obese patient can be challenging. In the next two steps, Dr Harry Thompson, Fellow Representative for the Society for Obesity and Bariatric Anaesthesia, SOBA and Dr John Cousins, founder of SOBA, discuss the anaesthetic techniques that can be used to safely manage the airways of this challenging patient cohort throughout the peri-operative period.
The terms bariatric and obese are often used interchangeably. Strictly speaking, bariatrics refers to the medical and surgical specialties dedicated to weight loss. In practical terms, when discussing the bariatric airway, we are referring to the management of the airway in obese patients who are undergoing general anaesthesia for any reason.
Obesity definitions and Prevalence
The World Health Organization divides obesity into classes depending on the body mass index:
| Class | BMI |
|---|---|
| Class 1 | 30-35 kg.m2 |
| Class 2 | 35-40 kg.m2 |
| Class 3 | >40 kg.m2 |
| Class 4 | >50 kg.m2 |
A limitation of body mass index is that it does not consider a person’s body frame and musculature. For example, a lean, muscular athlete might be deemed to be overweight or obese based on their body mass index alone. Measuring central obesity might be more appropriate as patients with more central, intra-abdominal distributed fat are at higher risk of perioperative events and are more likely to exhibit the metabolic syndrome. This distribution of intra-abdominal fat is referred to as the ‘apple’ body shape as opposed to the ‘pear’ body shape where the fat distribution is more peripheral:
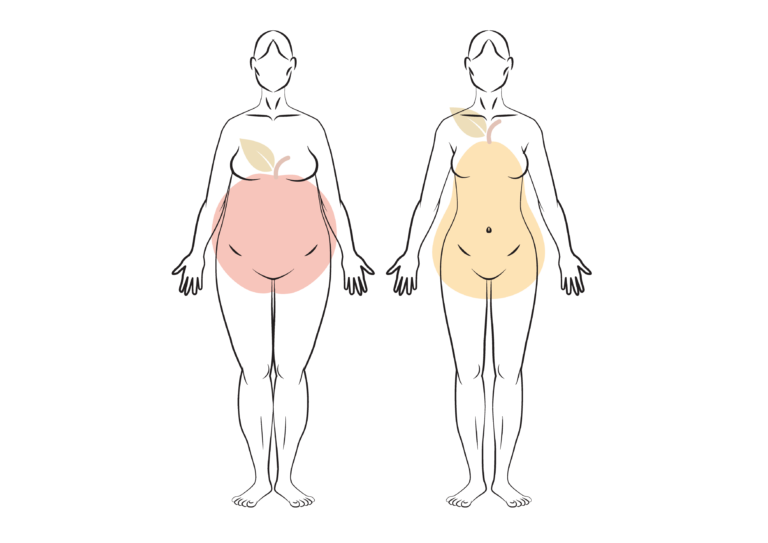
Waist circumference measurement is a method of screening for central obesity, being defined as a waist circumference greater than 88 cm in a woman and 102 cm in a man, or a waist to height ratio greater than 0.55.
In the US, irrespective of which definition is used, the rate of obesity is approaching 40% and most European countries are not far behind. As the rates of obesity increase, so do the number of obese patients presenting to hospital for both emergency and elective procedures.
Remember: obese patients are more likely to have other significant co-morbidities which can make them a very challenging patient group to manage,
Respiratory Physiology
Obesity has a significant impact on lung volumes, respiratory mechanics and gas exchange. The diagram below shows why the induction of anaesthesia leads to desaturation:
Obstructive Sleep Apnoea
Obstructive sleep apnoea (OSA) is the periodic partial or complete obstruction of the upper airway during sleep. It causes hypoventilation or apnoea. Acutely, this leads to poor quality sleep, daytime fatigue, poor concentration and headaches. In the longer term, it can lead to hypertension, left and right ventricular strain and eventually heart failure, pulmonary hypertension and arrhythmias.
In the perioperative period, OSA makes patients more at risk of:
- High sensitivity to opioids
- Airway obstruction in the first 24 hours after an anaesthetic
- Hypercapnia and ventilatory failure
The risk factors for OSA are very common in surgical populations:
- Age over 55
- Male gender
- Smoking history
- Alcohol use
- Upper airway pathology
- Neck Circumference
- Diabetes
- Family History
Because OSA is undiagnosed in a large proportion of the population, screening tests are very useful to raise suspicions and lead to further investigation. One such test is the STOP-BANG questionnaire (see table below). A formal sleep study (polysomnography) is required to categorise patients as mild, moderate and severe. Severe obstructive sleep apnoea, together with a large neck circumference, appears to correlate with a more difficult grade of laryngoscopy view.
| Symptom | Question |
|---|---|
| Snoring | Do you Snore Loudly (loud enough to be heard through closed doors or your bed-partner elbows you for snoring at night)? |
| Tired | Do you often feel Tired, Fatigued, or Sleepy during the daytime (such as falling asleep during driving or talking to someone)? |
| Observed | Has anyone Observed you Stop Breathing or Choking/Gasping during your sleep? |
| Pressure | Do you have or are being treated for High Blood Pressure? |
| BMI | Body Mass Index more than 35 kg/m2? |
| Age | Age older than 50? |
| Neck | Neck size large? (Measured around Adams apple) For male, is your shirt collar 17 inches / 43cm or larger? For female, is your shirt collar 16 inches / 41cm or larger? |
| Gender | Gender = Male? |
Low risk = 0-2, intermediate risk = 3-4, high risk = 5-8
Now we have examined some of the medical problems associated with obesity, let’s move onto the uniquely difficult airway of the obese patient in the next step.


Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.




