
How do we diagnose fungal disease? – Part 1

Fungal infections can be a diagnostic challenge resulting in overuse of antifungals. This is particularly the case with systemic fungal infections with high mortality.
A spectrum of diagnostic tests is available, but the interpretation of the results can be tricky as colonisation with the most common opportunistic fungal pathogens is common.
Therefore, these tests should only be used in the presence of clinical suspicion based on detailed patient history and assessment.
Clinical assessment and findings

Detailed history, examination and medical background is needed to determine if a fungal infection is likely (and if so which one), and to be able to distinguish colonisation from infection.
Below are some clinical features that are relevant to fungal infection:
Medical background – the key here is to identify an increased risk for opportunistic fungal infections. These include conditions that impair the immune system such as inflammatory diseases, immune deficiencies, diabetes and HIV. In the case of systemic fungal infections, the presence of lines and other indwelling medical devices or parenteral feeding are important. Ongoing sepsis increases gut permeability and risk for candidaemia. Recent invasive procedures (such as GI surgery) can lead to a fungal infection.
Drug treatments – Immunosuppressive medication (including topical, inhaled and systemic steroids, and chemotherapy) increase our suspicion of opportunistic infection. Recent or current antibiotic therapy can disrupt normal bacterial flora and increase the risk of candidosis.
Environmental contacts – Various exposures relevant to the presentation need to be considered. Many fungal pathogens are associated with specific contacts linked to their favoured environment.
- Use of sports facilities (athlete’s foot)
- History of skin trauma which has become contaminated with soil or vegetation (subcutaneous mycoses)
- Extensively damp and mouldy home (aspergillosis)
- Travel history, close contact with pigeon, chicken or bat droppings (cryptococcosis, histoplasmosis)
Travel history – Some of the systemic mycoses are endemic to specific areas of the world. For example, recent travel to midwest USA (coccidioidomycosis) or South America (paracoccidiodomycosis) would impact your differential diagnosis.
Sampling

The first step in fungal laboratory diagnostics is sample collection.
- Swabs can be used if Candida is the main suspected pathogen but skin scrapings, nail clippings or hair roots (bulb) are needed for the diagnosis of dermatophyte infections.
- Sputum is a useful sample when respiratory fungal infections are suspected, although BAL is preferred if invasive disease is suspected.
- Biopsies are very useful samples for the diagnoses of subcutaneous and deep fungal infections.
- CSF is the essential sample when a fungal CNS infection is suspected.
- Blood and other sterile site fluids are important samples for the diagnosis of systemic fungal infections. However, few fungi beside Candida species grow in blood culture. For other fungal pathogens, specific antigen tests and PCR can be performed. Fungal serology and fungal biomarkers can be also detected from blood samples.
Good quality specimens with detailed information are essential for good quality results. In general, fungi are more difficult to culture than bacteria and the intensity of infection (number of organisms per e.g. ml of BAL or blood) is significantly lower. For this reason, a larger volume of samples is recommended.
Microscopy and fungal culture
Often, confirming the diagnosis of a fungal infection relies on visualising and culturing the organism. Therefore, the first step in mycological laboratory diagnostics is microscopy whenever appropriate for the sample type. This is done alongside culture. Microscopy can provide a rapid confirmation of presence of fungi and the type seen (yeast/mould), which is very useful for guiding antifungal therapy.
Most fungi can be grown in a similar fashion to bacteria. However, some fungi are difficult to culture and it is not rare that fungal culture fails to recover the organism even if some were seen in microscopy. This is often due to incorrect processing or inadequate periods of incubation. Some fungal pathogens have specific growth requirements and they can only be detected if grown appropriately. It is therefore essential to communicate with the laboratory if a fungal diagnosis is suspected, so that the appropriate techniques can be used.
 Trichophyton verrucosum on agar plate
Trichophyton verrucosum on agar plate 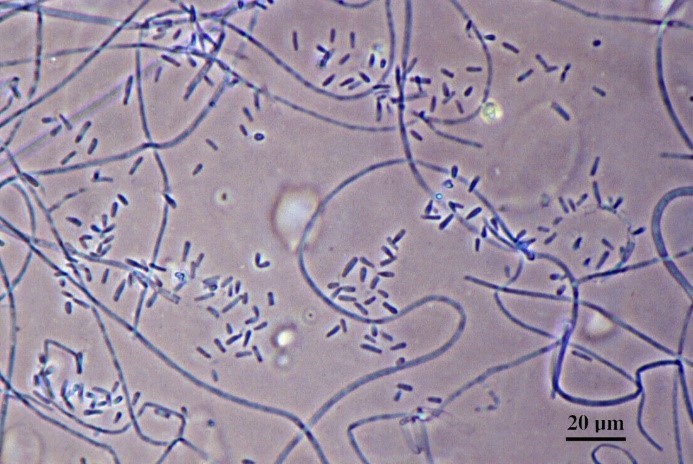 Trichophyton verrucosum under the microscope
Trichophyton verrucosum under the microscope
Fungal PCR
PCR can aid the diagnosis of fungal infection. However, it is important to understand that fungal PCR has a number of challenges including low intensity of infection and the need to process high volumes of sample as well as the hard to break fungal spores. Therefore, the sensitivity of fungal PCR is not necessarily much better than that of culture. Molecular techniques are particularly useful with the difficult to culture species and sample types.


Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.




