
How do we diagnose Invasive Aspergillosis? – Part 1
Diagnosing invasive aspergillosis (IA) is a challenging prospect. As a normally innocuous environmental fungus, Aspergillus can contaminate laboratory samples and colonise the oropharynx, sinuses and endotracheal tubes. The more sensitive methods are used for its diagnosis, the more difficult it often is to interpret a positive result.
Symptoms are often non-specific, or can be confused with a more common bacterial lower respiratory tract infection:
- Fever
- Cough (dry cough)
- Shortness of breath
- Pleuritic pain
- Haemoptysis
However, a combination of radiology, microbiology and clinical diagnostics can be used to aid early diagnosis:
CT scan of the chest
- Often preceded by a plain chest X-ray to exclude more common bacterial pneumonia, but which is not helpful in the diagnosis of IA
- The typical “halo sign” (nodular lesion surrounded by a “halo” of ground glass changes) is suggestive of IA in early infection
- Many other CT findings are associated with IA: large nodules, alveolar consolidation, ground glass opacities
- Diagnosis will rarely be made solely on radiology
Broncho-alveolar lavage (BAL)
- BAL samples can be subject to a number of tests
- Microbiological culture can isolate causative bacteria or isolate Aspergillus species
- Aspergillus PCR can detect presence of Aspergillus species within the secretions
- Galactomannan can also detect the presence of Aspergillus (or other fungi) in BAL fluid
Microscopy
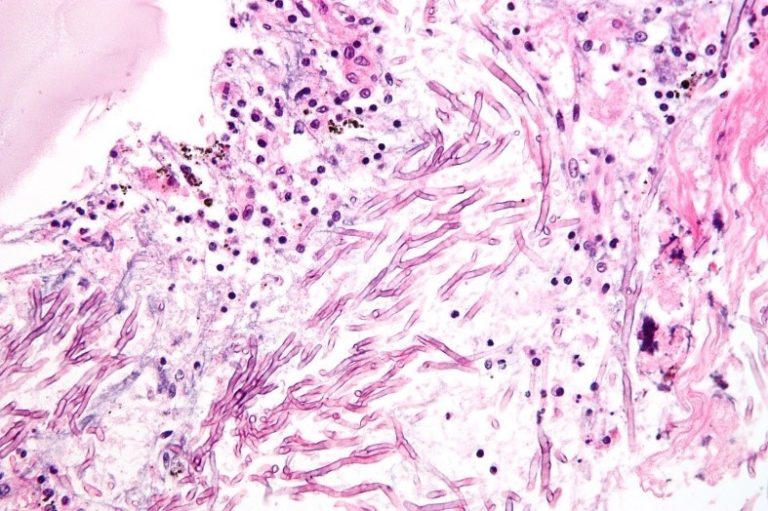 Above, Aspergillus hyphae seen under the microscope, in human tissue
Above, Aspergillus hyphae seen under the microscope, in human tissue
- Microscopy of respiratory samples can be very useful
- Biopsy sampling is not always possible, risks of the procedure need to be considered
- Fungal hyphae invading host tissue confirms a diagnosis of IA
- Low sensitivity (≈50%), IA cannot be ruled out based on microscopy alone
- Low specificity for Aspergillus as hyphae of other moulds may be indistinguishable from Aspergillus
Fungal culture
- Fungal culture can be done from respiratory samples or biopsy (if taken). Growth of Aspergillus species supports the diagnosis of IA. However, sensitivity is not high.
- Culture is valuable as susceptibility testing is recommended in all cases.


Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.




