
Quality improvement in action

As we have heard from Dr Robson, the high rate of adverse events in hospital patients has driven us to improve practice, reduce errors and understand near misses as well as other factors such as litigation costs, increased length of stay and risks.
Within the area of managing infection, interventions involving invasive medical devices and compliance with local policies for both infection control and antimicrobial prescribing are a focus for quality improvement.
There are several quality improvement methodologies used in healthcare, e.g. the Model for Improvement, LEAN, Six Sigma, but all use similar components.
The Model for Improvement provides a simple, yet powerful tool for accelerating improvement based on three fundamental questions:
- What are we trying to achieve? A clear aim – what, how much, by when?
- How will we know that change is an improvement? Measuring processes and outcomes.
- What changes can we make that will result in an improvement?
- What do we want to test? What can we learn as we go along?
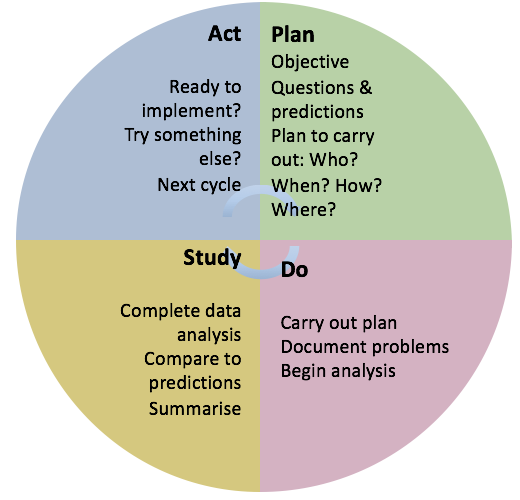
The Model uses PDSA (PLAN, DO, STUDY, ACT) cycles to test changes which may result in improvement. It is useful to consider PDSA as an ongoing process as shown in this diagram:
If you would like to learn more about quality improvement methodology in healthcare we suggest you use the following resources for further reading:
Institute for Healthcare Improvement
In Week 5 we will return to quality improvement methodology.
Now let’s think a bit more about how measurement for quality improvement could be applied to antimicrobial stewardship.
We can use process measures which are easy to collect to tell us if steps in the system are performing as planned.
- Are all clinical staff aware of the local antibiotic policy and able to access it at the point of care?
- Are all patients receiving the correct antibiotic as specified in the local policy?
However, outcome measures that measure the impact of changes made on patients are more valuable but also more difficult to collect.
- Are the antibiotics used effectively treating a specific infection? e.g. clinical cure rate/ mortality/ ICU admission.
We will now apply quality improvement methodology to clinical practice relevant to the outbreak scenario.
Aim
By the end of October 2015 all patients undergoing urology surgery in Dunswood Hospital will receive the correct antibiotic for surgical prophylaxis.
Measures
- Availability of antibiotic policy in all theatres where urology surgery is performed.
- Surgeons, anaesthetists and other theatre staff aware of antibiotic policy and can access it.
- Adequate stock of the policy antibiotic is available in all theatres used for urology surgery.
- Patients undergoing urology surgery are prescribed and administered the policy antibiotic at the correct time prior to the procedure.
Note that these are all process measures. The surgical site infection rate for patients undergoing urology surgery is an example of a longer term outcome measure.
Tests
- Display/locate policy in all relevant theatre areas and check still available daily.
- Engage with all staff to ensure they are aware of the policy and know where to find it in theatre – test methods of communication e.g. email, face-to-face, phone call, clinical meetings.
- Stock of antibiotics checked by theatre staff daily/weekly or topped up by Pharmacy staff daily/weekly.
- Audit antibiotic prescription and administration documentation in patient medication chart/notes. Test each change with one member of staff initially, then expand to several staff ensuring each change is tested in all staff groups and all theatres.
It is important to remember that some tests will fail and not have the desired outcome, but this is still useful learning and helps to think of new tests to improve practice.
“I did not fail one thousand times; I found one thousand ways how not to make a light bulb.” (Thomas Edison)
Antimicrobial Stewardship: Managing Antibiotic Resistance

Antimicrobial Stewardship: Managing Antibiotic Resistance
Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.




