
Measurement for quality improvement

Measurement has been used for centuries in research but more recently has become a cornerstone of benchmarking and scrutiny within healthcare.
It is also utilised through various methodologies to improve quality and failure rate in manufacturing industries and these approaches have become widely used in healthcare.
Data capture is a key factor in designing measurement of stewardship interventions. Electronic systems can capture data to provide quantitative information for monitoring longitudinal trends, but for many healthcare interventions manual collection of data through clinical audit may be required to support improvement in practice.
The use of quality improvement methodology within healthcare has expanded rapidly over the past ten years. This started in the United States with several healthcare providers addressing deficiencies in their systems, which were leading to high litigation costs, supported by the Institute for Healthcare Improvement (IHI). Quality improvement in healthcare is now widespread across Europe, North America, Canada and Australia. Much of the experience and the tools used in quality improvement originated in the manufacturing and aviation industries, which have radically improved safety during the past 25 years.
We have already considered why measurement is important, but when we want to start collecting data we need to think carefully about our specific reasons for collecting it, as this will inform the type and quantity of data we need to collect.
There are three reasons for collecting data:
- Research to generate evidence
- Accountability – judgement or scrutiny of performance
- Quality improvement
This table compares the important factors in deciding which type of data we need:
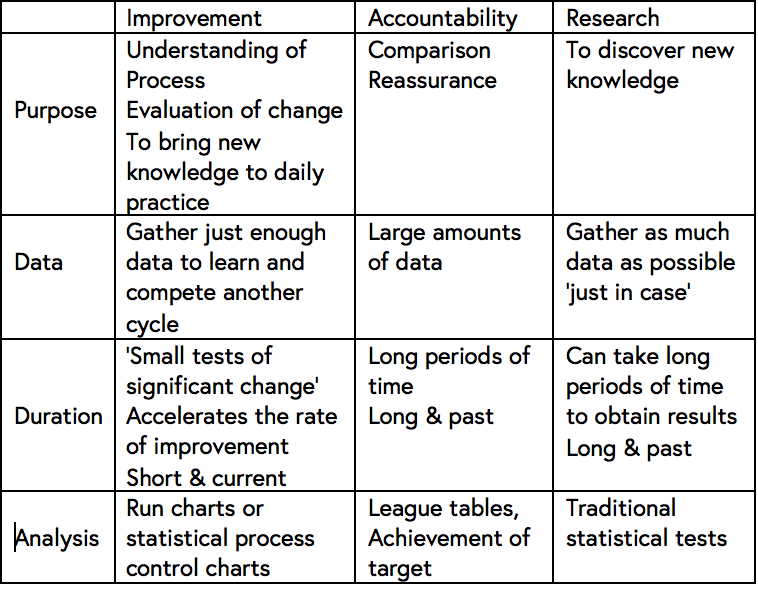
As you read this, consider which of these approaches would be the most appropriate to deal with the extended-spectrum beta-lactamases (ESBL) outbreak scenario?
IMPROVEMENT – frequent real time data collection may help to prevent spread and identify any risks due to non-compliance with infection prevention and antimicrobial use policies.
ACCOUNTABILITY – if this is not an isolated incidence of ESBL infection it may be useful to set targets for wards or hospitals to ensure compliance with infection prevention and antimicrobial use policies.
RESEARCH – as with all emerging infections, research is essential to gain a better understanding of how resistance spreads and which measures are most effective in containing them.
There is no right answer in the case of the ESBL outbreak, as all approaches would be suitable, but each will need different lengths of time to have an impact.
If an urgent change in practice were required, then the improvement approach would be best as this can start to have an impact on a small scale in a matter of days. For this to be effective, it would need to be focused in one ward, initially working with a small group of staff and carrying out many small tests of change.
For larger scale changes data collection for accountability may be better, with audits over several wards and feedback to staff. This will take time to establish a baseline, set targets and regular re-audit to determine if practice is changing.
A research approach may be useful, perhaps in addition to the other two, because it has the potential to generate robust data about the impact of changes on both process and patient outcomes. This would be a long-term objective and would require resources to implement.
So, although each may be useful, in the short term the improvement approach can rapidly make patient care safer and reduce the risk of further spread.
Antimicrobial Stewardship: Managing Antibiotic Resistance

Antimicrobial Stewardship: Managing Antibiotic Resistance
Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.




