
Exercise Limitations in Chronic Obstructive Pulmonary Disease

Chronic obstructive pulmonary disease is a highly prevalent condition characterized by airflow obstruction that reduces the ability to sufficiently empty the lungs. In the following two steps, we look at exercise intolerance in this clinical cohort, talk about the benefits of exercise, and present exercise guidelines.
Exercise Intolerance in Chronic Obstructive Pulmonary Disease
Exercise intolerance is a troublesome manifestation of chronic obstructive pulmonary disease (COPD). People with COPD are prematurely limited during maximal exercise as a result of the uncomfortable sensation of exercise. They can show:
- Reduced responses of peak oxygen uptake (VO2)
- Reduced peak minute ventilation (ie total volume of air entering the lungs per minute) and heart rate
- Slower rate of increase in oxygen uptake (VO2 kinetics) during submaximal exercise
- Increased anaerobiosis (muscle hypoxia or lack of oxygen), demonstrating a lactate threshold at relatively low work rates [1]
Exercise intolerance is closely linked to impairment/disability and is a stronger predictor of poor quality of life and survival than either lung function (measured by spirometry) or levels of blood oxygen.
Exercise intolerance in people with COPD results from a complex interaction between:
- Symptoms of dyspnea (shortness of air) and leg fatigue
- Ventilatory and respiratory mechanics impairment
- Pulmonary gas exchange limitations leading to arterial hypoxemia (low levels of oxygen in the blood)
- Peripheral muscle dysfunction
We will now look at the key concepts associated with exercise intolerance in COPD; dynamic hyperinflation of the lungs and peripheral muscle dysfunction.
Dynamic Hyperinflation of the Lungs
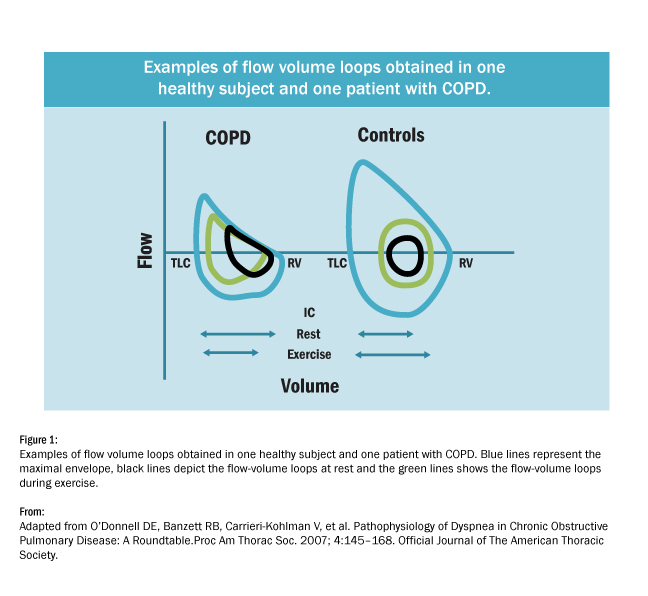
- For individuals with normal lung function, the end-expiratory lung volume decreases by approximately 200 to 400 ml with moderate exercise.
- In contrast, in patients with COPD, expiratory flow is limited at rest, and when breathing frequency is increased during exercise they have less time to breathe out. So, air is accumulated in the lungs increasing end-expiratory lung volume and reducing inspiratory capacity. This is called dynamic hyperinflation of the lungs (Pepin et al, 2007).
As you can see from in diagram below, the end-expiratory lung volume in the control or healthy participant is reduced during exercise (green line) compared with rest (black line), whereas it is increased in the participant with COPD. This dynamic hyperinflation leads to diaphragm weakness and may contribute to dyspnea and reduced exercise tolerance.
Peripheral Muscle Dysfunction
In addition to the damaging effect on the lungs, COPD contributes to skeletal muscle dysfunction which contributes to the exercise intolerance in COPD. This is characterized by a diminished peripheral muscle strength, muscle atrophy and muscle weakness. As you can see in the diagram below (Gea et al, 2013) lack of physical activity appears to be the main contributor to peripheral muscle dysfunction; whereas pulmonary hyperinflation seems to play the key role contributing to respiratory muscle dysfunction as mentioned above.
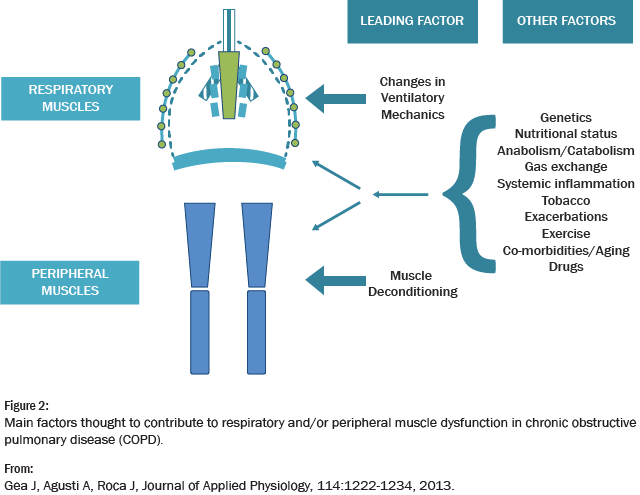
However, additional systemic factors, such as tobacco smoking, systemic inflammation, intense exercise, exacerbations, nutritional and gas exchange abnormalities, anabolic insufficiency, comorbidities and drugs also modulate muscle function.
Benefits of Exercise for COPD
Major benefits of supervised exercise training include increased physical capacity, decreased anxiety about breathlessness, greater independence in daily activities, reduced fatigue and improved quality of life. These positive outcomes occur even though impaired lung function continues to persist after exercise training.
In the next step we will be looking at exercise guidelines for COPD including inspiratory muscle training, neuromuscular electrical stimulation and high intensity interval training.
[1] However, in severe COPD the development of anaerobiosis does not show a disproportionate increase in minute ventilation. Thus, detection of a ventilatory threshold (the point at which ventilation starts to increase at a faster rate than VO2) may not be possible.
Exercise Prescription for the Prevention and Treatment of Disease


Exercise Prescription for the Prevention and Treatment of Disease
Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.




