
Early experience with nurse-led Linezolid monitoring
These slides describe our early experiences of specialist nurse-led Linezolid monitoring within our OPAT service.
Method
A service evaluation was performed. Patients were identified by review of OPAT service records. Clinical information was extracted from the hospital’s electronic patient results system. Data was recorded and analysed using Excel. Descriptive statistics are presented with the X2 test or Yate’s X2 test used to compare differences between groups.
Results
Since November 2010, 70 patients have been referred to the service (74% male, 26% female; age range 15 to 85 years). All patients were reviewed by a trained OPAT specialist nurse (also an independent prescriber) and had bloods taken weekly with medical review individualised to each patient’s underlying infection and ongoing needs.
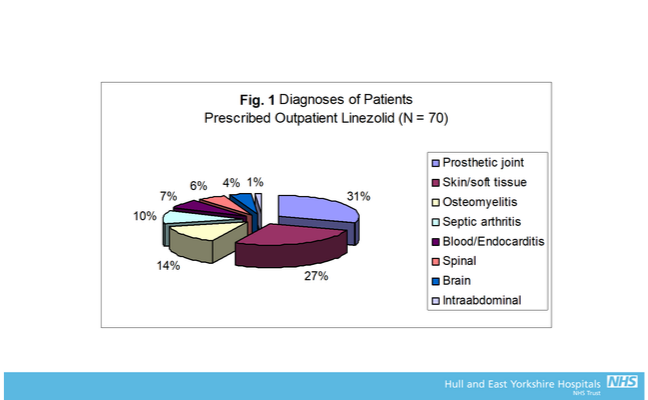 Figure 1.
Figure 1.
Treatment duration varied from 1 to 13 weeks; median = 4 weeks. Diagnoses of patients prescribed outpatient Linezolid are shown in Fig.1.
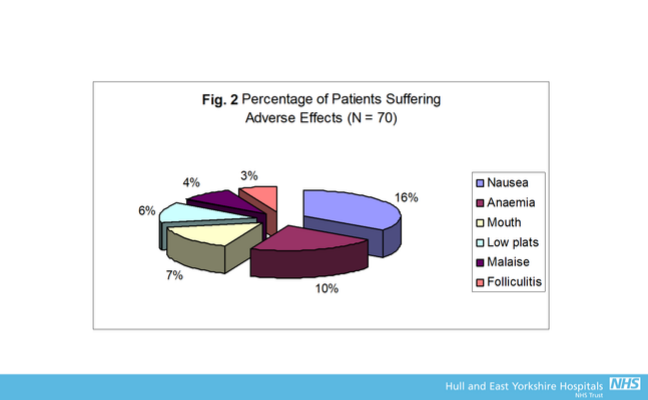 Figure 2.
Figure 2.
37% of patients suffered at least one adverse effect. The percentage of patients suffering specific adverse effects is shown in Fig.2.
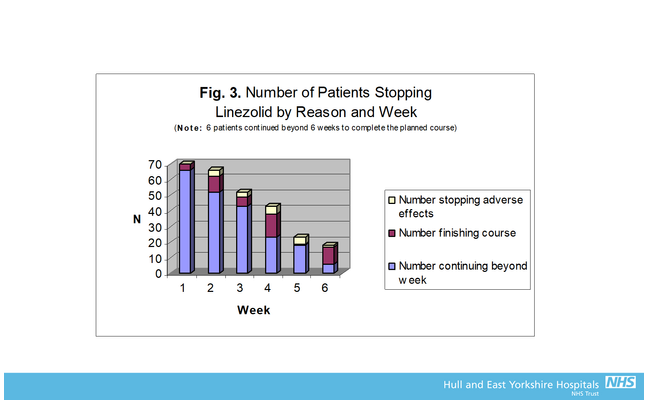 Figure 3.
Figure 3.
Most patients (76%) completed the intended course of Linezolid, but 21% changed to an alternative regimen and 3% stopped early. The most common reasons for changing/stopping Linezolid were severe nausea (35%) and low haemoglobin (22%). Fig. 3 shows why patients stopped Linezolid by week.
Two patients required hospitalisation for blood transfusion. In both instances, haemoglobin levels continued to fall in the 2 weeks following discontinuation of Linezolid.
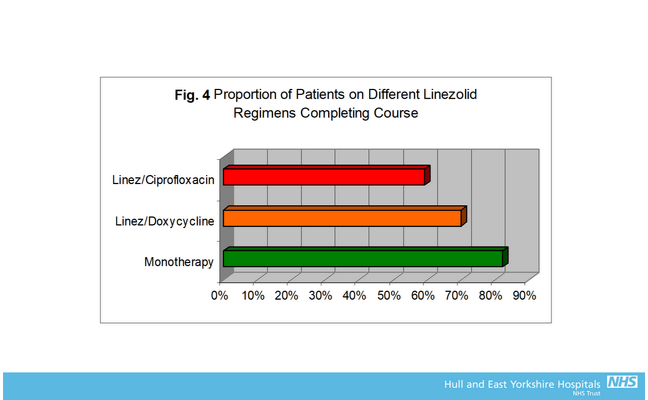 Figure 4.
Figure 4.
44% of patients received combination therapy; most commonly with Ciprofloxacin (24%) and Doxycycline (14%). A higher proportion of patients completed the planned course when receiving Linezolid monotherapy compared to those also taking Ciprofloxacin or Doxycycline (82% versus 63%; X2 test = 3.04, p = 0.08); see Fig. 4.
Age was the strongest predictor of completion of therapy with 93% (N = 29) of those under 60 years compared to 63% (N = 41) of older patients completing the planned course of Linezolid; X2 test = 8.14, p = 0.0004.
A higher proportion of male patients (81% versus 61% in females; Yate’s X2 test = 1.84, p = 0.17) completed their planned course of Linezolid; this did not appear to be due to differences in mean age or use of concomitant antibiotics.
Conclusions:
-
Nurse-led Linezolid monitoring via an OPAT service is feasible allowing the early detection of, and response to, adverse effects.
-
Two patients (3%) suffered progressive symptomatic anaemia after stopping therapy requiring readmission to hospital and blood transfusion, emphasising the importance of post-completion monitoring in those who develop anaemia.
-
Most patients completed the planned course of Linezolid. Age was the strongest predictor of non-completion; this did not appear to be due to differences in measured potential confounders between age groups.
-
When using Linezolid, concomitant antibiotic therapy is probably best avoided whenever possible.
Do our findings align with your experiences? Comment your experiences of monitoring Linezolid (if any) and discuss with your fellow learners.
Intravenous to Oral Switch: Within Outpatient Parenteral Antibiotic Therapy (IVOST)


Intravenous to Oral Switch: Within Outpatient Parenteral Antibiotic Therapy (IVOST)
Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.




