
Age Awareness

Chronic Condition Considerations
As humans age, the risk of chronic conditions increases.
It should be noted, that if an older adult has one chronic condition they are at an increased risk of suffering from several chronic conditions.
This has implications across many aspects of the older adults life in general, such as mobility, morbidity, medications, quality of life.
The following is a list of medical professionals that you might refer a client to:
- General Practitioner (GP)
- Physiotherapist
- Dietician
- Podiatrist
- Chiropractor
- Nutritionist
- Exercise Physiologist
- Occupational Therapist.
The diagnosed condition may be the same BUT:
There can be varying degrees, reactions to the condition, levels of fitness, ages, progression of the condition and motivation level of client.
Note!
Diagnosis V’s Referral – We can never diagnose a condition, but we can refer!
Rheumatoid Arthritis
“Arthritis is a condition affecting the synovial joint and is characterised by inflammation of joint structures and pain. Finding a balance between rest and PA has been a challenge. Despite traditional beliefs that exercise should be avoided, regular PA ↑ impairment & ↓ joint function without aggravating the system.”
Rodan, G.A. (1997)
Rheumatoid arthritis
- A chronic inflammatory disorder affecting the synovial joints on both sides of the body
- Involves an acute inflammatory reaction in the synovial membrane lining the synovial joint
- Chronic inflammation and swelling of the joints stretches and weakens ligaments
- Begins between the ages of 20 and 40 years with females more affected than males
- Client will experience joint pain
- Trigger for this is unknown although there is some relationship with bacteria or viral infections
- Can run in the family
- Joint deformity is very common
- Over time the synovial membrane can thicken, forming a pannus (granulation tissue)
- The bone under this pannus can be eroded
- Fibrosis is the end result of inflammation
- Client goes through exacerbations and remissions
- During a severe flare up the client may feel stiff during the entire day whereas during a remission period the stiffness may be limited to the morning, and sometimes the client experiences.
Aim at maintaining/improving:
- Joint ROM
- Muscular Flexibility
- Muscular Strength
- Endurance
- Cardiovascular Fitness.
Osteoarthritis
- Degenerative joint disease
- Pain and stiffness
- Usually > 65 years old
- Not systemic
- Triggered by many factors, e.g. injury, overuse.
Physical Activity & OA
- Aim: to improve ROM and prevent further decrease in mobility
- Aquatic exercises reduce impact and stress on the joints
- Cycling also reduces joint stressors
- Consider osteoarthritis in the hands – avoid exercises or sports that require a tight grip.
Exercise prescription – Arthritis
- Flexibility/ROM every day
- Vigorous activity is contraindicated when there is acute inflammation
- Allow ample warm up and cool down – joint fluid temperature
- Explain to the client that some discomfort may be experienced, does not mean further damage, stop when discomfort becomes painful
- Incorporate functional exercises (ADL’s) – sit-to-stand & step ups
- Aerobic exercise: more than 150 min per week; 30-40% MHR for deconditioned; 40-60% MHR recommended; can start with short bouts – 10 min and progress; 3-5 times per week
- Resistance exercise: 10-15 repetitions (40-50% 1RM); 2-4 sets per exercise; target all major muscle groups; 2-3 times per week.
Osteoporosis
Osteoporosis is a condition in which the skeleton has become susceptible to low trauma fracture due to reduced bone mass. An increased propensity to fall in later life compounds the risk of an osteoporotic fracture.
Osteoporotic fractures afflict 60% of women and 30% of men over the age of 60 in Australia.
Osteoporosis often remains undetected until a person actually suffers a fracture. Any bone can be affected but the most common site is the spine. The most serious, debilitating and costly osteoporotic fracture, however, occurs at the hip.
- A degenerative joint disease causing pain in the affected joints
- Commonly affects the hip and knee joints
- More common as age progresses
- Bone loss occurs at a faster rate than bone replacement
- Risk of fractures and falls
- Fractures after falls don’t always have a good prognosis.
Difference between RA and OA
Unlike RA, OA is not a systemic problem but simply degeneration of the joint actually affected. For this reason, it’s possible that one side of the body can be affected without the other side. Fatigue may occur from general lack of fitness that results from pan and inactivity. It is characterised by:
- Erosion of articular cartilage
- Sclerosis (thickening or hardening) of bone underneath the cartilage (subchondral Sclerosis)
- Formation of bone spurs (osteophytes) which grossly alter the bony contours & enlarge the joint, leading to possible subluxation of the bone from the joint (extreme circumstances only).
Causes of osteoporosis can be hereditary, as well as there being a natural tendency to begin to lose bone tissue around the age of 30-40 years. Other factors that increase bone loss and the risk of osteoporosis are:
- Reduced circulating oestrogen i.e. Menopause (and as occurs with chronic training-related energy imbalance)
- Inactivity and immobilisation (e.g. Sedentary lifestyle, bed rest or casting)
- Some medical conditions & / or their treatments (eg. Glucocorticosteriods)
- Slim individuals may also be at risk since low levels of body fat are associated with poor bone mineral density
- Amenorrhoea: A problem for Young female athletes who compete in sports where appearance is important e.g.. Gymnastics or marathon running
- Postmenopause: Due to a lack of female hormones which affects bones
- Increases the risk of fractures from falls and even coughing
- Paralysis or immobilisation: 1% decrease in bone density per week
- Underweight: low levels of BF associated with poor bone mineral density
Vitamin D: aids in calcium absorption
Risks for osteoporosis
- Lack of physical activity
- Paralysis or immobilisation
- Alcohol abuse
- Excessive caffeine intake
- Amenorrhoea & post menopause
- Poor diet (calcium/Vit D), smoking and alcohol abuse
- Underweight/Low body fat levels.
Reading Please read the following article, Arthritis (osteoarthritis) and exercise
Prostate Cancer
Prostate cancer develops when abnormal cells in the prostate gland grow more quickly than in a normal prostate, forming a malignant tumour. Prostate cancer is the most common cancer diagnosed in Australia and the third most common cause of cancer death. One in 6 men will be diagnosed with prostate cancer by the age of 85. It is more common in older men, with 63% of cases diagnosed in men over 65 years of age.
The symptoms can include:
- Frequent urination, particularly at night
- Pain on urination
- Blood in the urine
- A weak stream.
The more widespread disease often spreads to the bones and gives pain or unexplained weight loss and fatigue.
Exercise prescription – Prostate Cancer
General Guidelines:
- Flexibility/ROM everyday
- Add pelvic floor exercises
- Be aware of fatgue related to treatment modalities
- Incorporate functional exercises (ADL’s) – sit-to-stand & step ups.
Aerobic exercise: 20-60 mins per session, 60-90% of MHR, RPE 13-15 on the Borg’s Scale, 3-5 times per week
Resistance exercise: 6-12 repetitions (40-50% 1RM); 6-8 exercises, 3 sets per exercise; target all major muscle groups; 2 or more times per week.
Reading Please read the following article, Prostate Cancer and exercise
Pelvic Floor & Incontinence
Incontinence is a term that describes any accidental or involuntary loss of urine from the bladder (urinary incontinence) or bowel motion, faeces or wind from the bowel (faecal or bowel incontinence).
Incontinence is a widespread condition that ranges in severity from ‘just a small leak’ to complete loss of bladder or bowel control. In fact, over 4.8 million Australians have bladder or bowel control problems for a variety of reasons. Incontinence can be treated and managed. In many cases, it can also be cured. Having strong pelvic floor muscles gives us control over the bladder and bowel. Weakened pelvic floor muscles mean the internal organs are not fully supported and you may have difficulty controlling the release of urine, faeces (poo) or flatus (wind).
Common causes of a weakened pelvic floor include childbirth, obesity and the associated straining of chronic constipation. Pelvic floor exercises are designed to improve muscle tone and prevent the need for corrective surgery.
What are pelvic floor muscles?
Pelvic floor muscles are the layer of muscles that support the pelvic organs and span the bottom of the pelvis. The pelvic organs are the bladder and bowel in men, and bladder, bowel and uterus in women. The pelvic floor muscles stretch like a muscular trampoline from the tailbone (coccyx) to the pubic bone (front to back) and from one sitting bone to the other sitting bone (side to side). These muscles are normally firm and thick.
Imagine the pelvic floor muscles as a round mini-trampoline made of firm muscle. Just like a trampoline, the pelvic floor is able to move down and up. The bladder, uterus (for women) and bowel lie on the pelvic floor muscle layer.
The pelvic floor muscle layer has hole for passages to pass through. There are two passages in men (the urethra and anus) and three passages in women (the urethra, vagina and anus). The pelvic floor muscles normally wrap quite firmly around these holes to help keep the passages shut. There is also an extra circular muscle around the anus (the anal sphincter) and around the urethra (the urethral sphincter).
Although the pelvic floor is hidden from view, it can be consciously controlled and therefore trained, much like our arm, leg or abdominal muscles.
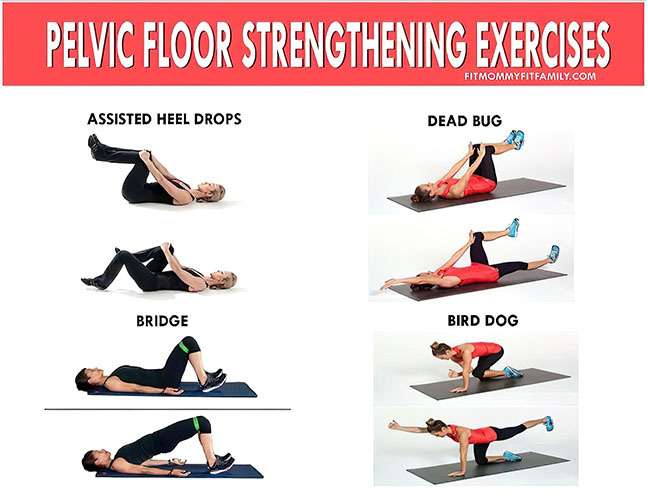
Exercise prescription & pelvic floor
- Pelvic floor exercises should be completed several times per day
- Try to maintain abdominal brace for up to 10 seconds
- Then relax and rest for 15-45 secs before next attempt
- Repeat
- Bracing can be completed lying down, upright sitting and/or standing.
Readings
Please read the following article, The Continence Foundation
Personal Trainer's Toolkit: Developing Fitness Programs for Older People


Personal Trainer's Toolkit: Developing Fitness Programs for Older People
Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.




