
Sample types for testing
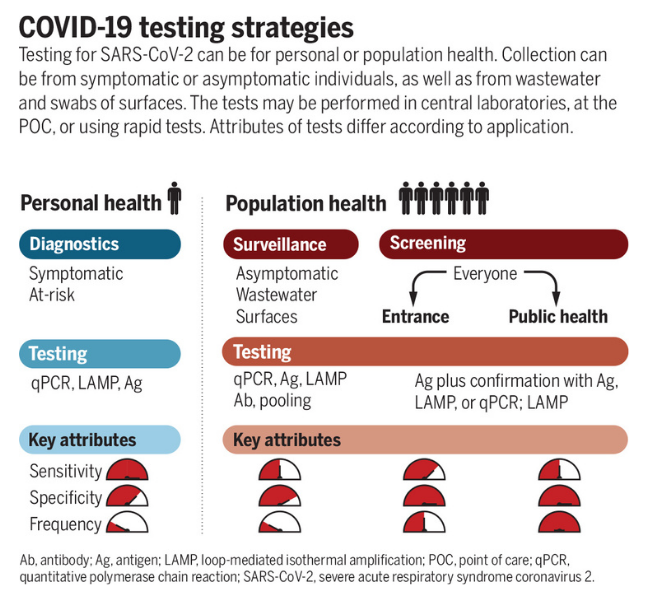
When deciding what type of sample to use for detecting SARS-CoV-2, there are a number of considerations. Is the test for clinical diagnosis or community surveillance? Do you want to sequence the subsequent sample after detection? How tolerable is the test to the population you are targeting? Thinking about the health question you are trying to answer will guide both the sample type used and the testing technique employed (Figure 1).
Click here to enlarge
Figure 1 – COVID-19 testing strategies. Testing for SARS-CoV-2 can be for personal or population health. Collection can be from symptomatic or asymptomatic individuals, as well as from wastewater and swabs of surfaces. The tests may be performed in central laboratories, at the POC, or using rapid tests. Attributes of tests differ according to application. Source Science
Decisions made at the sampling stage may impact the utility of downstream data. Saliva samples might be easier and less distressing to collect from particular groups (such as children, the elderly and the clinically vulnerable), but may exhibit reduced sensitivity for detection and insufficient RNA for sequencing. Wastewater sampling can provide sufficient RNA for sequencing and variant detection in the community but does not provide individual-level data.
Sensitivity, specificity and prior probability
For each test, there will be a given sensitivity and specificity. Sensitivity is the proportion of true positive results detected by the test. For clinical diagnostic tests, the aim should be to have a very high sensitivity to reduce the number of false-negative missed cases. The specificity is the proportion of true negative results reported as negative by the test. Again, the aim is for this to be as high as possible to reduce false positives, however, the balance for public health benefits might tolerate a slight reduction in specificity to ensure maximal sensitivity. This balance will change depending on the setting and disease (Figure 2). The performance of each test will also be impacted by the prior probability of an individual being infected. For example, a result is less likely to be a false positive in a person with symptoms and known exposure to a possible case as opposed to someone screened at random. To see how these three values impact on each other you can alter the values on a COVID-19 test accuracy calculator.

Click here to enlarge
Figure 2 – Sensitivity results for the PCR test in stool/rectal swabs (A), urine (B), blood (C), sputum (D), saliva (E) and nasopharyngeal aspirate/swab and throat swab (F). Source: American Journal of Infection Control
Sample type comparison
The primary consideration if considering a particular sample type for clinical diagnostic testing should be that it delivers the correct result for the individual at the detection stage. This will allow appropriate interventions such as isolation or treatment. Secondary to this are sequencing considerations which provide population health level data. The best samples will achieve both of these criteria.
Many studies have been conducted to evaluate the merits of different sample types; the results of the sensitivity analysis from a metanalysis conducted early in the pandemic are shown in Figure 2. From this study, we can see that sputum samples give the highest sensitivity for SARS-CoV-2 PCR detection with a pooled sensitivity of 97% (95% confidence interval (CI) 90-100). The worst performing sample type was urine with a pooled sensitivity of 0% (95% CI 0-4). You can also see that there is significant variation between studies, reinforcing the benefits of a meta-analysis approach when considering implementing change rather than relying on individual trials.
Additional considerations for sequencing
Both viral detection and sequencing require a sufficient quantity and quality of RNA to be present. Depending on the sequencing technique used, there may or may not be an amplification step. High-quality sequencing data is more readily achieved from samples with a cycling threshold (Ct) value of less than 30. However, this is not fully quantitative and will vary between diagnostic platforms. Also, some platforms do not deliver a Ct value which makes sample selection for sequencing more challenging. A combination of this lack of Ct value and instability of sample buffer means that certain point-of-care diagnostic assays are not well suited to subsequent sample sequencing.
From Swab to Server: Testing, Sequencing, and Sharing During a Pandemic


From Swab to Server: Testing, Sequencing, and Sharing During a Pandemic
Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.




