
Disclosure and non-disclosure
Here we are talking specifically about two situations: where DVA has been disclosed, and where DVA has not been disclosed but is suspected.
The women/birthing persons discloses an experience of DVA
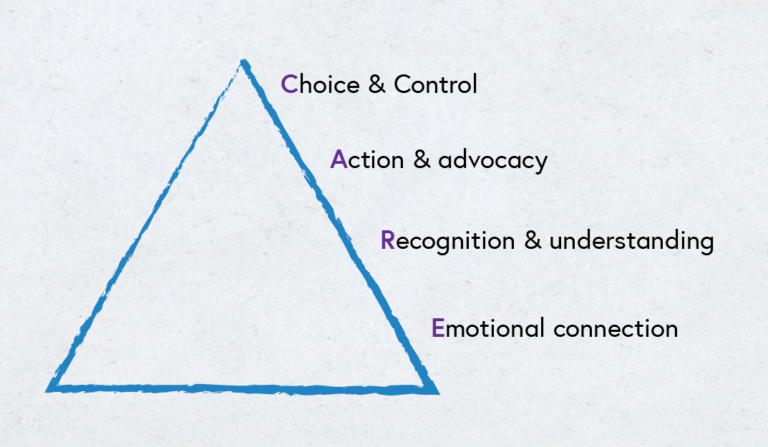
Based on a review of the literature on what women want after disclosing DVA, Tarzia et al., 2020 developed the CARE model:
Select the image to expand it.
(Adapted from Tarzia et al., 2020)
It recommends emotional connection, practical support through action and advocacy, and an approach that emphasises the person’s autonomy and individualised needs.
Woman- or person-centred care is about employing good listening skills, showing compassion and paying attention to non-verbal behaviours and cues. Ensuring privacy and confidentiality (and explaining about the limits of confidentiality) is also essential as part of a frontline response and will encourage the person to elaborate and discuss their concerns and experiences with you.
We will look at appropriate responses in further detail later in the course, starting with Validate the person’s experiences.
DVA is suspected but the person does not disclose
Follow the LIVES approach and avoid pressuring the person in any way.
They should be offered resources and information, and ideally, a follow-up appointment. Supporters can experience a sense of disappointment when people choose not to disclose the abuse or disclose it but then decline to take any action.
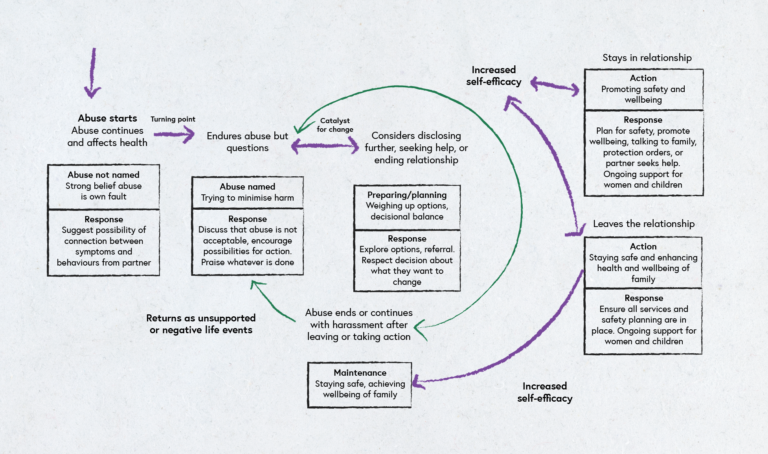
Offering compassion and support over time can assist a person to move through different stages of readiness (Reisenhofer & Taft, 2013). These stages include the victim/survivor acknowledging the abuse (‘naming’ it as such), recognising links between mental/physical health problems and the abuse; understanding the risks they and their baby/other children face; preparing for change and taking action (for example making a safety plan, leaving the partner).
A prerequisite for a person to accept help is their awareness or recognition that what is experienced is abuse. Inquiry and validation of experiences and feelings can assist the disclosure process over time. Empowering people to make even small changes can increase their self-efficacy with regard to addressing the abuse.
You can assist a person to make links between their health status and the abuse by asking: ‘Can we explore how your partner’s behaviours may be affecting your health/your pregnancy/your baby/your children? Have you had any thoughts on this?’
Often, this interaction sows the seeds; arranging a follow-up may allow further exploration of the person’s experiences in their relationship.
Select the image to expand it.)
(Adapted from García-Moreno et. al., 2015)
The figure above from García-Moreno et. al., 2015 is a helpful representation covering appropriate responses for the different stages of readiness for change experienced by those exposed to DVA.
Research and references
García-Moreno, C., Hegarty, K., d’Oliveira, A. F. L., Koziol-McLain, J., Colombini, M., & Feder, G. (2015). The health-systems response to violence against women. The Lancet, 385(9977), 1567-1579. DOI link.
Mauri, E. M., Nespoli, A., Persico, G., & Zobbi, V. F. (2015). Domestic violence during pregnancy: Midwives׳ experiences. Midwifery, 31(5), 498-504. DOI link
Reisenhofer, S., & Taft, A. (2013). Women’s journey to safety—the Transtheoretical model in clinical practice when working with women experiencing intimate partner violence: A scientific review and clinical guidance. Patient Education and Counseling, 93(3), 536-548. DOI link
Tarzia, L., Bohren, M. A., Cameron, J., Garcia-Moreno, C., O’Doherty, L., Fiolet, R., Hooker, L., Wellington, M., Parker, R., Koziol-McLain, J., Feder, G., & Hegarty. K. (2020). Women’s experiences and expectations after disclosure of intimate partner abuse to a healthcare provider: A qualitative meta-synthesis. BMJ Open, 1011, Article e041339. DOI link
Taylor, J., Bradbury‐Jones, C., Kroll, T., & Duncan, F. (2013). Health professionals’ beliefs about domestic abuse and the issue of disclosure: A critical incident technique study. Health & Social Care in the Community, 21(5), 489-499. DOI link
World Health Organization. (2019). Caring for women subjected to violence: A WHO curriculum for training health-care providers. Web link
Identifying and Responding to Domestic Violence and Abuse (DVA) in Pregnancy


Identifying and Responding to Domestic Violence and Abuse (DVA) in Pregnancy
Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.




