
Awake Tracheal Intubation – DAS Guidelines
In this video, Dr Imran Ahmad, as one of the Guidelines authors, takes a few moments out of his operating list to discuss the key recommendations from the DAS Guidelines on Awake Tracheal Intubation.
As we have seen, awake tracheal intubation (ATI) is a safe technique for patients with difficult airways. Despite this, we know that it is used in as few as 0.2% of all intubations in the UK. The traditional approach, using a flexible bronchoscope, is an advanced technique which requires training and regular practice to maintain skills. The equipment is costly and relatively difficult to maintain. As most clinicians do not perform ATI on a regular basis, they may feel reluctant to use the technique even when it is indicated.
These guidelines aim to demystify awake intubation and lower the threshold for using the technique in patients with difficult airways. They provide clear guidance on decision making, preparation and performance of the commonly used techniques. They include advice on oxygenation, sedation, topicalisation, set up and performance, how to adapt the technique according to the patient circumstances such as the critically ill, obstetric and obese and what to do if difficulties are encountered.
The full publication [1] includes visual aids to help with human factors and ergonomics, here are some examples:
Cognitive aid: Sedation-Topicalisation-Oxygenation-Procedure (STOP)
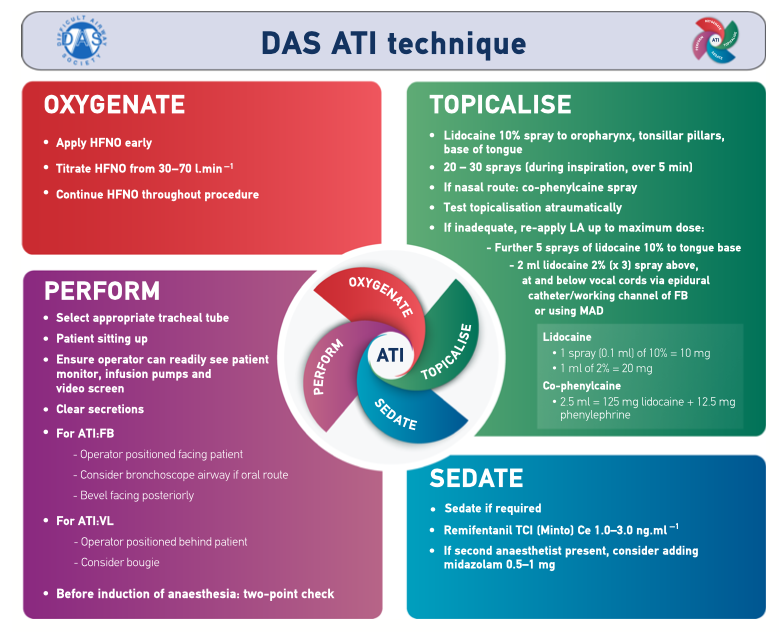 HFNO: high-flow nasal oxygen. LA: local anaesthetic. FB: flexible bronchoscopy. MAD: mucosal atomising device. TCI: target-controlled infusion. Ce: effect-site concentration. VL: videolaryngoscopy. ©Difficult Airway Society 2019.
HFNO: high-flow nasal oxygen. LA: local anaesthetic. FB: flexible bronchoscopy. MAD: mucosal atomising device. TCI: target-controlled infusion. Ce: effect-site concentration. VL: videolaryngoscopy. ©Difficult Airway Society 2019.
Examples of ergonomics for awake tracheal intubation
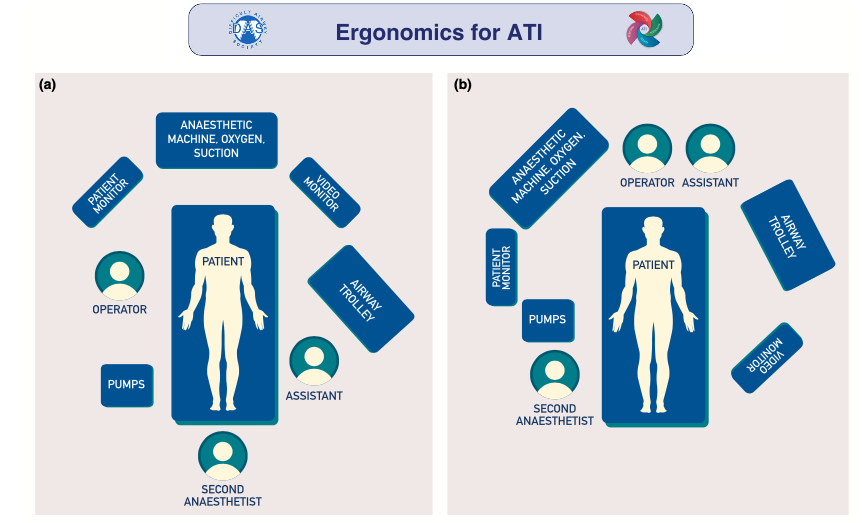 ©Difficult Airway Society 2019. (a) Awake tracheal intubation performed with the operator positioned facing the patient who is in a sitting up position. (b) Awake tracheal intubation performed with the operator positioned behind the supine/semi-recumbent patient. This figure forms part of the Difficult Airway Society guidelines for ATI in adults and should be used in conjunction with the text below.
©Difficult Airway Society 2019. (a) Awake tracheal intubation performed with the operator positioned facing the patient who is in a sitting up position. (b) Awake tracheal intubation performed with the operator positioned behind the supine/semi-recumbent patient. This figure forms part of the Difficult Airway Society guidelines for ATI in adults and should be used in conjunction with the text below.
The primary operator should have a direct line of sight of the patient, video monitor and patient monitor, as well as immediate access to infusion pumps, anaesthetic machine, suction and oxygen delivery device.
If a second anaesthetist is present, they should be positioned with a direct line of sight of the patient and have immediate access to infusion pumps, as well as be able to access all other equipment.
The anaesthetic assistant’s primary position should be with immediate access to the airway trolley, and in proximity to the operator.
An ATI checklist is also provided
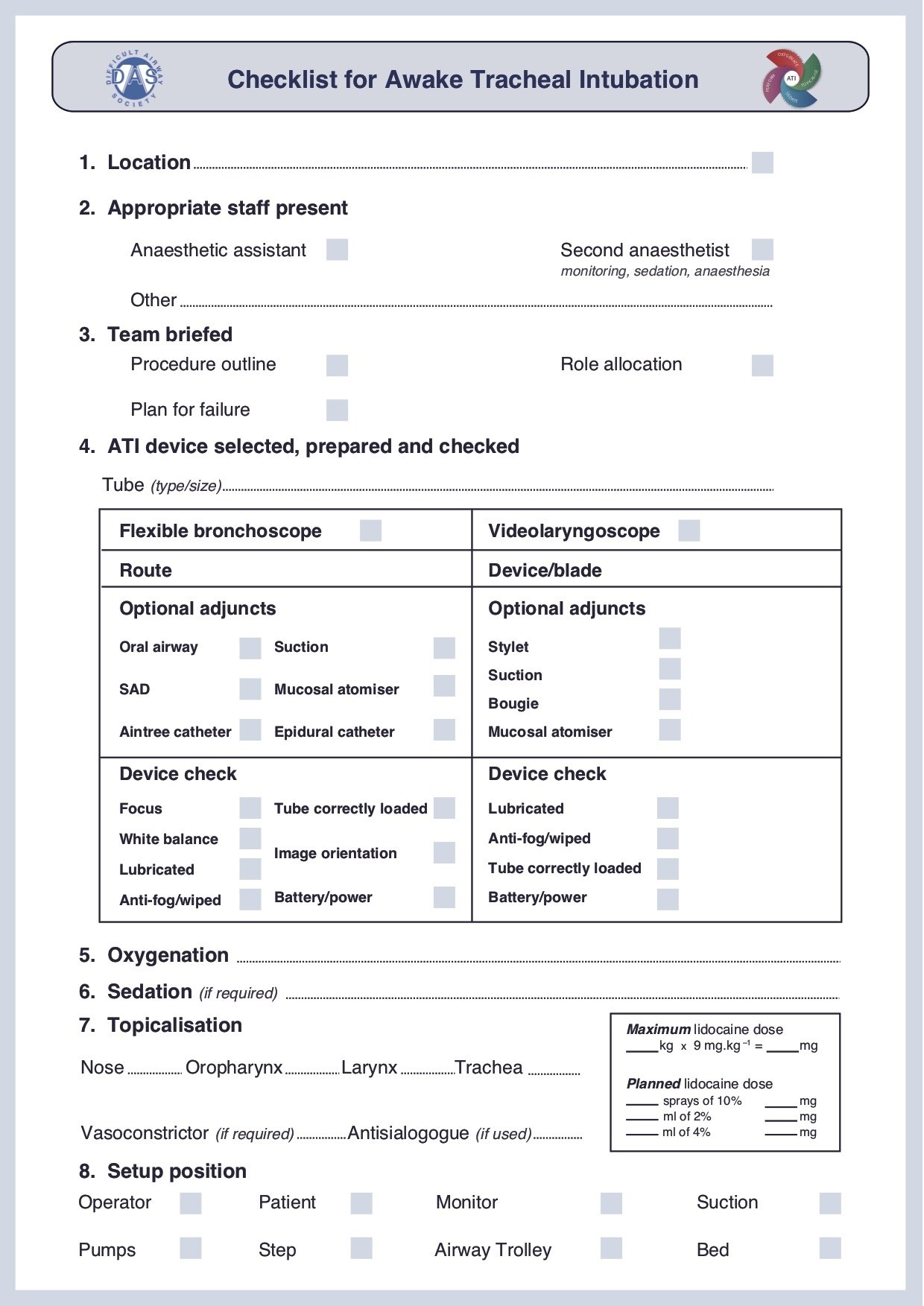 ©Difficult Airway Society 2019
©Difficult Airway Society 2019
How confident are you at performing or assisting in an awake tracheal intubation? Do you use a checklist before you start? Do you have the anaesthetic room laid out as suggested above? Do you think you might try this next time? Please do discuss this with your fellow learners before going onto the next step, exploring jet ventilation.
References


Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.


