
Vision Rehabilitation for Diabetic Eye Disease

As you read this article, consider the range of support requirements and interventions available to a person with low vision due to diabetes.
A retired teacher Mr Solomon, who is 64 years old, has low vision due to diabetic retinopathy despite having had laser treatment. He cannot read his newspaper, sign documents or watch television anymore. He finds it difficult to be outside when the sun shines. He has stopped using his mobile phone because he cannot read the messages. He uses insulin and cannot draw out the dosage and feels very dependent on his wife and children. He is bored, anxious and feels down.
There are many people with diabetic retinopathy, all over the world, who are in a similar situation to Mr Solomon. They have suffered substantial vision loss despite being treated for their diabetes and eye problems. Life can become a struggle for the individual with low vision.
The World Health Organization defines a person who needs to be assessed for low vision care as someone “who has impairment of visual functioning even after treatment and/or standard refractive correction, and has a visual acuity of less than 6/18 down to and including light perception, or a visual field of less than 10 degrees from the point of fixation, but who uses, or is potentially able to use, vision for the planning and/or execution of a task.” In every day practice the WHO definition is broadened to “A person with low vision is one who has an impairment of visual function for whom full remediation is not possible with conventional spectacles, contact lenses or medical intervention and which causes restriction in that person‘s everyday life” (UK Low Vision Services Consensus Group 1999). This definition includes, but is not limited to, those who fall under the WHO definition and focuses on the reduced ability to carry out important activities for daily living.
What needs to happens to a person with low vision?
The care for people with low vision due to diabetes is still mainly medical. Often, there is limited awareness (even amongst eye health professionals) that people can greatly benefit from low vision care and vision rehabilitation, including counselling. Close collaboration with, and referral to and from, low vision and community based rehabilitation services and organisations for people with disabilities will ensure that more can be done after visiting the eye health or diabetes clinic.
Low vision: Assessing persons with diabetes
Patients with diabetes have many special needs that are related to the use of vision, for example :
- To fill insulin syringes
- Read labels on medicine bottles
- They may also have tingling or numbness, which affects their hands and feet, making it difficult to handle their injections, monitor their blood sugar levels or take care of their feet.
It is important to consider 4 key areas for assessment and interventions of people with low vision due to diabetic retinopathy.
The four key areas for assessment and intervention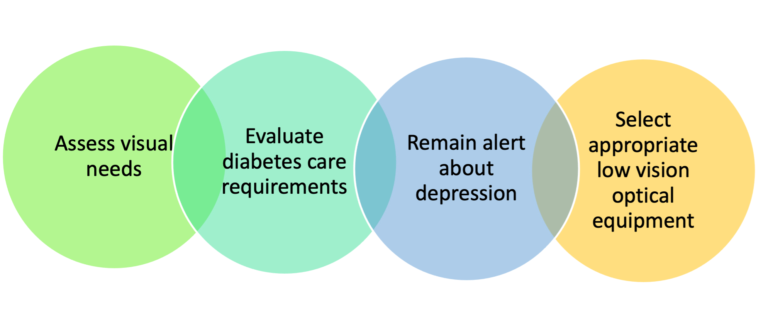
1. Visual needs
Additionally to loss of visual acuity, they may also experience :
- Vision changes due to blood sugar fluctuations
- Sensitivity to glare (e.g., not able to walk around safely when the sun shines)
- Their vision levels may fluctuate during the day
- Loss of contrast sensitivity is common, and this may affect many daily activities such as recognising friends, outdoor mobility, sewing and, cooking
- Loss of colour vision, especially blue-yellow loss
- Visual field loss, either central or peripheral field loss, or a combination of the two, results in e.g., difficulty reading labels and newspapers and walking around
All these visual functions should be assessed both in the eye health low vision clinic and in daily life activities by community-based services in the clients’ own environment (at home, school, work).
2. Care of diabetes
Investigate what the patient needs to use their vision for to manage their diabetes: e.g., for injecting insulin, blood glucose monitoring and foot care. What would be the best methods to use, taking into consideration the patient’s vision and the support they may have at home or even in their work environment.
3. Depression
Anxiety and depression is not uncommon in persons with diabetic retinopathy. Many patients benefit from support and counselling to learn to deal with the combined impact of vision loss and diabetes, and their increased dependence on others.
4. Low vision related/vision rehabilitation interventions
a. Non-optical measures and environmental adaptations
- Control of light: Reduce glare outdoors by wearing a cap, using an umbrella or wearing sunglasses outside. Increase light, using a well-directed reading lamp, for tasks such as cooking or reading.
- Increase contrast (and use colours to create good contrast) in and around the house and at work. Use dark tape around a light switch; cut coloured vegetables on a white or very dark surface; put dark stones or plants on the sides of the light-coloured paths around the patient’s house.
- Organise a cupboard with food items in a way that is good for the individual client, e.g. sequence items alphabetically or use large size, good contrast labels – remember vision may fluctuate during the day.
- Mobility training: The first thing to learn by the person and a family member is what the most appropriate and safest way is of being guided around. This training can easily be given by eye health staff as they also need to guide patients in their clinic. Mobility training (without or with a cane) to move around more independently, is beneficial to many and increases independence and self-respect. Find out where this is available near the clients’ home.
Guidelines for eye health workers and other helpers assisting blind and visually impaired persons.
b. Optical interventions, such as magnifiers are especially helpful for near tasks such as reading books, magazines, labels and prices.
- Spectacles to correct refractive errors, including presbyopia, should already have been prescribed by the eye health services or clinical low vision service.
- Telescopes are useful for distance tasks such as watching television.
- For clients with central visual field loss, it may be necessary to first learn to use eccentric viewing to learn to look around areas of decreased vision, before starting to use magnification. Find out who can provide this kind of training; low vision services should be able to help.
- After the low vision professional has determined how much magnification is needed, the kind of device that helps the client to do the activities he or she needs and wants to do can be discussed. The main question to ask is: “For what activity is it needed?”
For distance tasks: Is a telescope required for watching TV or for watching sports outside?
For near tasks, the following needs to be considered, together with non-optical interventions:
- Simple hand magnifiers are often used for reading labels, recipes, prices.
- Stand magnifiers may be good for longer periods of reading.
- Should the device be hands-free, e.g. to draw up insulin? Spectacles with a high + diopter lenses for magnification mean a patient can keep both hands free.
- Does the device need to provide additional lighting? Illuminated hand or stand magnifiers may help.
A case study:
How can low vision and rehabilitation services support Mr Solomon?
His best corrected distance visual acuity is 6/36. With a 3x telescope he can watch TV at a distance of at least 2 metres, see most of the TV screen and he now does not block the view of other household members.
His near vision was 3.2M (size of a large headline) at 25 cm. He was first prescribed +3.00 dioptres reading glasses. He can now read 2M at 25 cm, a size that is 2x smaller than 4M.
He was prescribed and taught to use 2 different magnifiers:
1. A +24.0 D illuminated stand magnifier with which he can read even the smallest print in newspapers
2. A 24.0D hand magnifier for reading his mobile phone, seed packets, medicine labels and prices. He also uses it to find the place where he needs to sign a document.
Handheld magnifiers are useful for many tasks and are easily portable. 
He was advised to wear a cap to reduce glare from the sun. Advice on improving lighting and contrast in his house was given by a visiting staff member of a community-based organisation for people with disabilities. He now feels much more independent and is a happier person. The family members are happier too!
Other considerations for selecting a device for near activities:
- Does the device need to give viewing choices (such as vertical and horizontal screen)?
- Does the magnification power need to be adjusted?
- Can the image be frozen to give more time to read or look?
Can colour and contrast be changed?
Some of these options are available in free mobile phone magnification apps (such as Smart Magnifier or Supervision+), and all are available in handheld video magnifiers (these last devices are expensive compared to mobile phone apps). The advantage of being able to adjust magnification power is that the amount of magnification can be changed if vision changes during the day. If these areas of intervention are addressed, most people with low vision due to diabetic retinopathy can perform many of the daily activities they used to do.
Diabetic Eye Disease: Building Capacity To Prevent Blindness

Diabetic Eye Disease: Building Capacity To Prevent Blindness
Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.




