
Opportunistic and systematic screening

As you read this article, consider which approach to screening is most suitable for your setting at present and what needs to be planned to manage diabetic retinopathy in your setting or in Ormo, our hypothetical case study?
Screening is not intended to be a diagnostic test. Patients with positive findings must be referred for further assessment. It is therefore very important that, prior to establishing any form of screening for sight threatening diabetic retinopathy (DR), that effective treatment services are already established – there is no point in screening for a condition that cannot be treated.
Key questions to consider before setting up a DR screening service in any health system:
- What is the best approach to find people with diabetes and offer them the screening test?
- How much will it cost to implement the screening and eye care services?
- What are the best approaches to reach people who face geographical and financial barriers to access screening?
Generally, we discuss approaches to screening as opportunistic or systematic.
Opportunistic screening
Opportunistic screening relies on early detection of disease in people who present to health care providers for various complaints. It involves examining eyes of people with diabetes when the opportunity arises e.g. when they attend a diabetes clinic for treatment or an optometrist for a general check-up.
Guidance and information for opportunistic screening needs to be sign posted at various levels of service delivery to raise awareness and guide persons with diabetes (often without any vision complaints) to seek an eye examination. For example, we can raise awareness about diabetic eye disease through primary health officers, general practitioners, pharmacists and diabetologists.
Realistically, awareness raising about eye examination for people with diabetes can only be carried out if the health system already has suitable treatment centres for referrals. For example in India, diabetes and eye screening camps are set up together to reach patients in rural regions. In some of these camps, trained technicians use mobile DR screening in an equipped van with a teleconnection to the base hospital to get guidance on patients found to have retinopathy.
Systematic screening
Systematic screening for diabetic retinopathy is organised at the population level. The basic steps are:
- Establishing a register of people with diabetes
- Managing a call and recall system
- Examination of the retina by trained and accredited personnel
- Applying standardised protocols for the detection and referral of people needing further examination and treatment
- Providing accessible, good quality treatment services.
The first evidence of the benefits of systematic screening came from a study in the 1990s which reported that the low prevalence of blindness in people with type 1 and type 2 diabetes in Iceland was due to the systematic screening programme established in 1980. A further report showed that the prevalence of legal blindness from DR amongst people with diabetes in Iceland dropped from 2.4% in 1980 to 0.5% in 2005. Reductions in the prevalence of blindness from diabetic retinopathy have also been reported following the introduction of systematic screening programmes in Sweden and Poland.
A systematic screening programme was introduced in England, Scotland Wales and Northern Ireland in 2002/2003 following research into the effectiveness and cost-effectiveness of systematic screening and reviews by the UK National Screening Committee and the Health Technology Board for Scotland.
In 2014, it was reported that in England and Wales, for the first time in at least five decades, diabetic retinopathy/maculopathy was no longer the leading cause of certifiable blindness among working-age adults in England and Wales.
Systematic screening can outperform opportunistic screening but it requires considerable investment. To implement systematic screening in the low- and middle-income countries where 80% of people with diabetes live will need cost effective strategies:
- The frequency of screening – should this based on the individual risk of developing sight threatening diabetic retinopathy, or on a standard interval for everyone?
- Increasing geographic reach through use of tele-screening models and portable/mobile technology.
- Taking the images using modern non mydriatic fundus cameras operated by trained technicians.
Setting up some approach to screening is essential for controlling DR in every health system: either opportunistic in low prevalence, low resource settings or systematic screening in high prevalence and/or high resource settings.
Four stages of setting up DR screening
DR screening programmes develop through four stages.
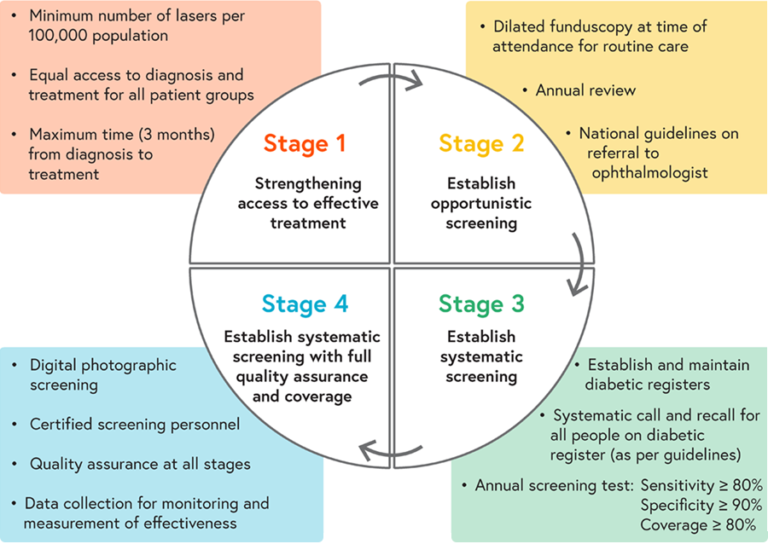
(Click to enlarge) Adapted from http://www.drscreening2005.org.uk
Stage 1: Strengthening access to effective treatment
- Minimum number of lasers per 100,000 population
- Equal access to diagnosis and treatment for all patient groups
- Maximum time (3 months) from diagnosis to treatment.
Stage 2: Establish opportunistic screening
- Dilated funduscopy at time of attendance for routine care
- Annual review
- National guidelines on referral to ophthalmologist.
Stage 3: Establish systematic screening
- Establish and maintain diabetic registers
- Systematic call and recall for all people on diabetic register (as per guidelines)
- Annual screening test: Sensitivity ≥ 80%, specificity ≥ 90%, coverage ≥ 80%.
Stage 4: Establish systematic screening with full quality assurance and coverage
- Digital photographic screening
- Certified screening personnel
- Quality assurance at all stages
- Data collection for monitoring and measurement of effectiveness
Is this four step approach to setting up screening applicable in your setting? If it is, which step is the starting point for your health system?
Diabetic Eye Disease: Building Capacity To Prevent Blindness

Diabetic Eye Disease: Building Capacity To Prevent Blindness
Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.





{kind=link}