
Tailoring Antimicrobial Resistance (TAP)
We have already looked at several implementation strategies for AMS. In this step, we will focus on another strategy – Tailoring Antimicrobial Resistance Programmes (TAP).
TAP is a new methodology developed by the World Health Organization (WHO) which uses a behavioural insights approach called Tailoring Health Programmes (THP). TAP not only aims to identify barriers to optimal behaviour but also identifies the incentives that drive such behaviour. TAP utilises the Behaviour Change Wheel and COM-B approach mentioned previously.
TAP is an evidence-based approach based on the belief that people’s health behaviours are rarely static, and are susceptible to change, both positive and negative. By unpacking health behaviours, and better understanding the multiple factors that facilitate or hinder their performance, the THP approach supports the design of interventions for lasting change.
This new initiative from WHO aims to apply the principles of implementation science and behaviour change to the context of developing, implementing and evaluating ASPs. Tailoring interventions towards the needs of specific groups (e.g. pharmacists, patients, prescribers, veterinarians) and contexts (e.g. communities, pharmacies, hospitals) can ensure that AMR interventions are effectively implemented and lead to positive behaviour change among populations .
What is it? Values, Principles & Process
TAP provides a stepwise guide on how to design and implement a behaviour change intervention for target-specific groups to address specific drivers of AMR.
The approach has been developed by the WHO as part of an overall vision of integrating people-centred research and social science methods into health programme planning and policy.
The process is premised on the understanding that health decisions are affected by social and individual contexts and that to influence behaviour or maintain best practice, different factors affecting an individuals’ behaviour must be understood and addressed.
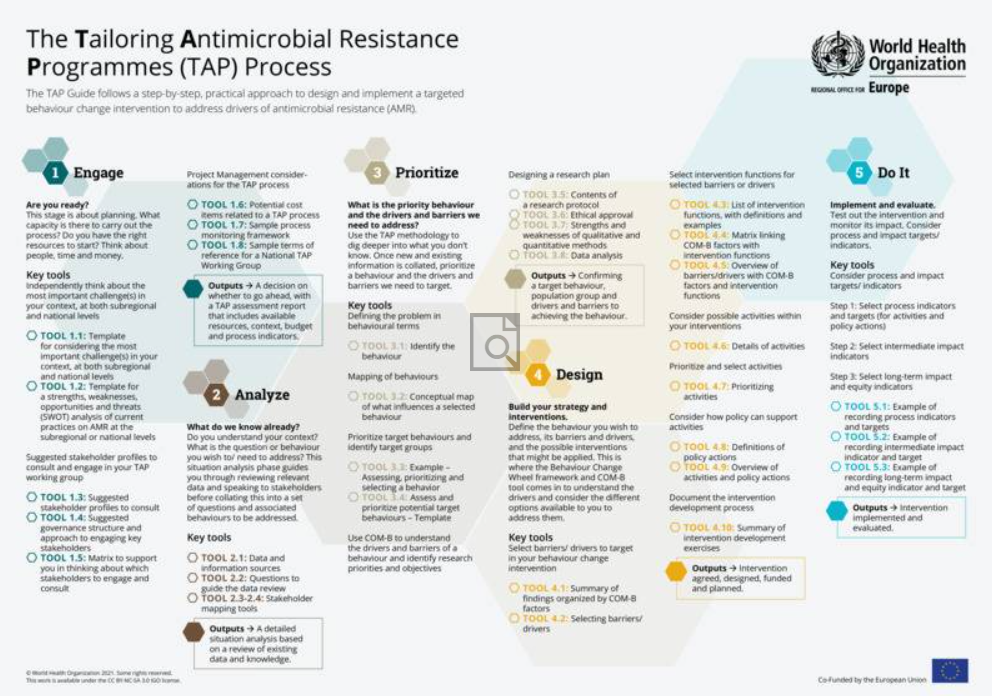
The TAP process consists of five stages, as shown in the diagram below, built on a set of core values and principles and supported by a peer-reviewed theoretical model.

These stages are:
1. Engage: Are you ready? – This stage is about planning. What capacity is there to carry out the process? Do you have the right resources to start? Think about people, and time and money needed and available, before you decide to go ahead and plan your process.
2. Analyse: What do we know already? – Do you understand your context? What is the question or behaviour you wish or need to address? This situation analysis phase guides you through reviewing relevant data and speaking to stakeholders before collating findings into a set of questions and associated behaviours to be addressed.
3. Prioritise: What is the priority behaviour to address? – Use the TAP methodology to dig deeper unto what you don’t know. Once new and existing information is collated, prioritise a behaviour and the drivers of and barriers to a target.
4. Design: Build your strategy and interventions – Define the behaviour you wish to address, the related barriers and drivers, and the possible interventions that might be applied. This is where the behaviour change wheel (BCW) and COM-B (Capability, Opportunity, Motivation – Behaviour) tools help you to understand the AMR-related behaviours and consider options available to address them.
5. Do it: Implement and evaluate. – Test out the interventions and monitor its impact. Consider adjusting as needed. If it works, scale it up!
The TAP process is built on a set of interrelated values and principles as shown below.

Click here to see a larger version of this image.
This infographic is also available as a screen-reader compatible PDF.
To systematically address drivers and barriers to AMR-related health behaviour, the TAP process is partially built on the Behaviour Change Wheel (BCW) model for understanding health behaviours in complex interventions. Employing the BCW model:
- Ensures a systematic and comprehensive approach to understanding public health behaviours and designing targeted interventions.
- Helps avoid blind spots in the process.
- Provides a structure for discussions, studies, analyses and prioritisation.
- Helps establish hypothesised causal pathways that describe how specific intervention components affect health behaviour and help identify effective interventions.
At the core of the BCW model is the Capability, Opportunity, and Motivation for Behaviour change (COM-B) framework. The BCW/COM-B model was chosen for the TAP because it takes a comprehensive approach to identify and address individual and contextual drivers and barriers to AMR-related behaviours.
The diagram below from the WHO TAP quick guide shows how this COM-B model can be applied to AMS interventions.

Click here to see a larger version of this image.
This infographic is also available as a screen-reader compatible PDF.
Resources
To help understand and utilise TAP, here are several useful tools and resources.
The World Health Organization have produced a poster highlighting the 5 steps of TAP implementation, including links to various tools to aid in its implementation.

Click here to see a larger version of this image.
WHO have also produced:
- The TAP Quick Guide, a step-by-step, practical approach to design and implement a targeted behaviour change intervention to address drivers of AMR
- The TAP Toolbox, a series of exercises and tools to work through 5 stages outlined in the TAP Quick Guide.
Hopefully, you now understand the fundamentals of TAP to begin to achieve proper antibiotic stewardship. Would TAP be a suitable approach to consider in your practice?’ Share your thoughts in the comments below!
How to set up an Antimicrobial Stewardship Programme


How to set up an Antimicrobial Stewardship Programme
Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.





{kind=link}
{kind=link}
{kind=link}