
How to use and monitor Co-trimoxazole – a brief primer

Co-trimoxazole is usually well tolerated in most patients without comorbidities or renal impairment, but it can have deleterious effects on renal function (and cause hyperkalaemia) for those on prolonged therapy, particularly those with existing chronic kidney disease.
Before starting this antibiotic the patient’s creatinine clearance is calculated by the Cockcroft-Gault equation based on a recent serum creatinine. A pre-therapy full blood count and liver enzymes are also required.
We usually use a dose of 960mg twice daily for most infections, but sometimes increase to 1.44g twice daily for severe or cerebral infections.
Patients with a creatinine clearance of between 15 and 30 mL/minute/1.73 m2 require dose reduction (by 50%) or an alternative antibacterial regimen (preferred option in our experience).
Co-trimoxazole is best avoided in those with a creatinine clearance below 15 mL/minute/1.73 m2 unless considered essential (e.g. Pneumocystis jirovecii pneumonia). Patients with diabetes and/or established chronic kidney disease and/or those who are prescribed any medication that has a tendency to increase serum potassium (e.g. ACE inhibitors, spironolactone, etc.) or cause renal impairment, need to be monitored carefully.
The predisposition of Co-trimoxazole to cause renal impairment and hyperkalaemia is well established due to the trimethoprim component (it is structurally similar to amiloride) so this aspect of the need for monitoring also applies to patients prescribed prolonged courses of Trimethoprim.
The patient’s current medications are checked for drug-drug interactions with each component of Co-trimoxazole before starting; Trimethoprim, in particular, interacts with many drugs including some antibacterials. For patients on Warfarin, the concurrent use of Co-trimoxazole can result in higher than anticipated prothrombin times (both components).
Co-trimoxazole also causes bone marrow suppression, although in our experience it is much less common than with Linezolid. Full blood count monitoring for those on prolonged therapy, however, is recommended. Alternative therapy should be considered for those already taking bone marrow suppressive agents (e.g. methotrexate) unless considered essential, in which case consideration should be given to the risk/benefit of stopping or decreasing the dose of the other agent (which may be required anyway to control the patient’s infection).
Patients are educated about the known predisposition of Co-trimoxazole to cause rash and/or itching and the risk of Stevens-Johnson syndrome and toxic epidermal necrolysis. In our experience, if patients are advised to stop Co-trimoxazole (and to contact the COPAT service) immediately on the onset of rash, then the rash subsides and does not progress.
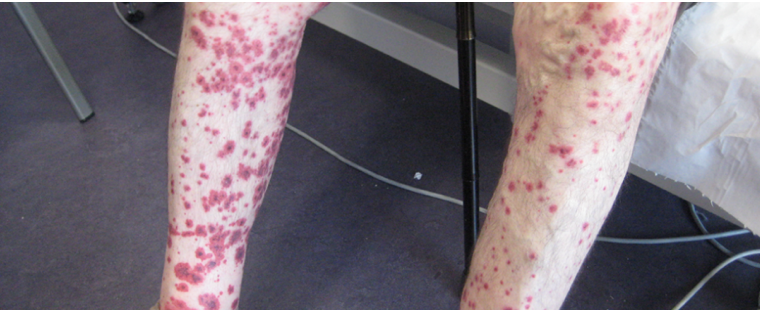
Vasculitis-type rash due to Co-trimoxazole – the patient was asymptomatic and it gradually resolved after stopping without harm.
Despite extensive inpatient and outpatient use at our hospital, we have not seen life-threatening rashes to date, although we do see mild to moderate rashes requiring cessation of therapy from time-to-time. Renal impairment and hyperkalaemia are more common and of more concern in our experience. Patients at risk of the above problems are reviewed in the COPAT service at 7 to 14 days after starting and then monthly thereafter or more frequently if at high risk.
Patients without comorbidities or drug-drug interactions require less initial monitoring and can be managed within a classical outpatient clinic environment (we recommend checking baseline bloods as above, however, and then no later than 4 weeks after starting and earlier if symptomatic adverse effects occur), although it should be noted that hyperkalaemia has been reported in patients without obvious risk factors. Other cautions, contraindications, drug-drug interactions and adverse effects can be reviewed via the resources in see also below.
Intravenous to Oral Switch: Within Outpatient Parenteral Antibiotic Therapy (IVOST)


Intravenous to Oral Switch: Within Outpatient Parenteral Antibiotic Therapy (IVOST)
Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.




