Home / Healthcare & Medicine / Care / A Journey Through Transfer Medicine / Equipment, Positioning & Drugs

Equipment, Positioning & Drugs
Due to the increased weight and dimensions of patients with obesity, modifications may be necessary to equipment, positioning and drugs.

© Dr James Shuttleworth, North Central London Adult Critical Care Transfer Service (NCL-ACTS)
Here we take a look at the equipment modifications that ensure a patient living with obesity is transported safely and comfortably, and raise your awareness of the important things to consider…
Equipment Limitations
- When undertaking a bariatric transfer, knowledge of the limitation of equipment used is vital. Various models of transport trolleys are available with weight limits, many of which can exceed 300kg.
- However, certain functions such as the hydraulic height adjustment function of the trolley may be limited above certain weight values.
- Not only should we consider the weight of the patient, but the weight of additional equipment that may be loaded onto the trolley must also be taken into account – and this may exceed 25kg.
- Given relatively high weight limits, trolley width is often the limiting factor. The trolley must be able to accommodate the widest point of the patient safely. Specialist bariatric trolleys have additional side rails, which help with this.
Moving & Securing The Patient
- If possible, patients should be encouraged to position themselves on the trolley.
- Transferring a patient onto a trolley should be planned in advance and may be made considerably easier with the use of inflatable sliding sheets, which must be removed from under the patient after transfer across. Here you can watch how this is operated.
- It is very important to secure the patient to the trolley properly, but care must be taken with patient restraint systems as the buckles can damage skin. If too tight, restraints can also cause peripheral nerve damage, impede ventilation and increase the risk of venous thrombosis.
- Silicone gel pads or extra pillows may be used to pad pressure areas such as elbows and heels.
A knowledge of the width of corridors and doors, as well as lift limitations will aid safe navigation through hospitals. Getting stuck can leave you in a dangerous and unexpected position with a critically unwell patient if not considered beforehand.
- Loading the trolley into the ambulance can be assisted greatly using winch systems (see image below) built into the ambulance that provide more control as well as reduce the risk of manual handling injuries to staff. Again, these have weight limits which should be checked before use.
Patient with obesity being loaded into ambulance using a winch system
Air Transfer
- When considering transfer via air, attention must be paid to the total weight that will be carried by the aircraft, as exceeding the weight limit could have devastating consequences.
- The limiting factor for air transfer will also include the dimensions of the patient, as many aircraft and helicopters will have a significant ‘step’ up to the loading surface or small doorways.
Ventilation
- Positive pressure ventilation of obese patients can be challenging and a transport ventilator that is able to provide high levels of feedback, as well as advanced ventilation modes, is advantageous.
- A trial period on the transport ventilator provides reassurance that the equipment is able to meet the patient’s requirements for the transfer and an arterial blood gas is advised prior to departure to confirm stable gas exchange.
Monitoring
- Non-invasive blood pressure monitoring may be difficult if using the upper arm and an appropriately sized cuff should always be used. Alternative sites include the forearm and calf.
- There should be a low threshold for invasive blood pressure monitoring, particularly for longer transfers or if a patient has any risk of cardiovascular instability.
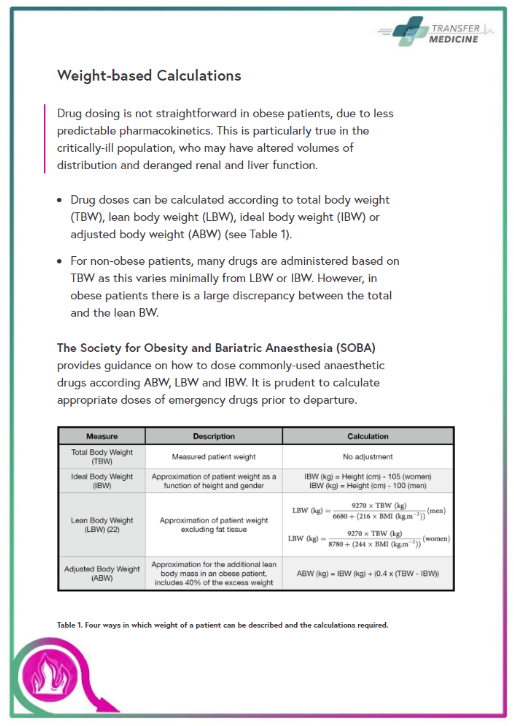
Drugs In Bariatric Transfers
- Medication in critically-ill patients with obesity presents a number of challenges, including correct dosing, unpredictable clinical effects and difficulties with intravenous access.
- Since high infusion rates of sedative agents may be required for obese patients during transfer, requirements should be calculated and adequate supplies of these agents should be available. It is recommended to take more than you need!
- Intravenous access is often difficult to establish in the obese patient and prone to displacement, which can lead to interruption of life-sustaining medications, such as vasopressors and to extravasation and soft tissue damage.
Have at least two peripheral cannulae or, ideally, a multi-lumen central venous catheter and check it’s secured and flushed prior to transfer. Remain vigilant to extravasation of drugs, which may be less obvious in the obese patient.
- Learn more about weight-based calculations
Awareness
- The Fifth National Audit Project (NAP5) found that patients living with obesity suffered a disproportionate incidence of awareness under general anaesthesia, particularly when neuromuscular blocking drugs were used.
Care should be taken to ensure patients are sufficiently sedated when using neuromuscular blockers.
© Dr James Shuttleworth, North Central London Adult Critical Care Transfer Service (NCL-ACTS)


Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.





{kind=link}
{kind=link}