
Linking Syndromic testing and AMS
Professor Manaf Alqahtani elaborates on AMS in this video, discussing the value syndromic testing — and diagnostic stewardship using syndromic testing — adds to existing AMS programs.
As Professor Alqahtani explains in the video, rapid molecular identification methods — such as syndromic testing — shorten the time taken to identify offending microorganisms. This can result in targeted antimicrobial therapy being given sooner for the appropriate duration, and can subsequently aid antimicrobial stewardship by encouraging efficient use of antimicrobials.
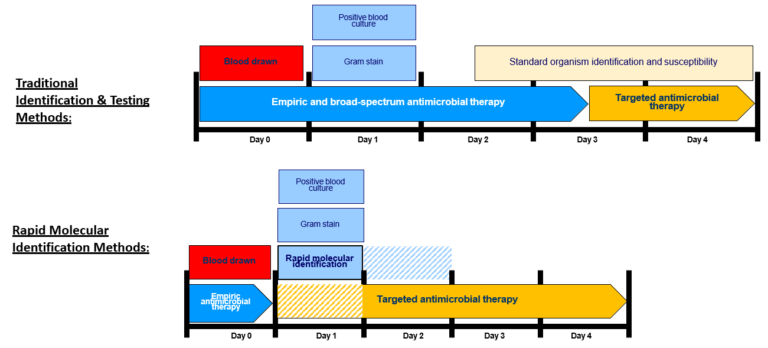 Organism Identification and Initiation of Targeted Antimicrobial Therapy: Traditional versus Rapid Molecular diagnostics for bloodstream infection – click here for a closer look
Organism Identification and Initiation of Targeted Antimicrobial Therapy: Traditional versus Rapid Molecular diagnostics for bloodstream infection – click here for a closer look
For more information and further reading on this topic, please see the see also section below.
Syndromic Testing and Antimicrobial Stewardship

Syndromic Testing and Antimicrobial Stewardship
Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.

