
Methods of diagnosis

How can we diagnose visceral leishmaniasis? A number of different methods have been developed over the years but not all are suitable for routine use in the field or clinic[1].
Any diagnostic test needs to be sensitive, specific, suitable for the region, practical, cheap and accessible. For example, in a well-equipped and resourced hospital laboratory invasive techniques and sophisticated methods may be routinely used, whereas in primary health care centres with basic facilities, a simple easy-to-use method needs to be employed.
The clinical case definition for VL is “a person from a known VL endemic area that presents with fever of more than 2 weeks duration and has splenomegaly and/or wasting and/or lymphadenopathy”. These features must be confirmed by a diagnostic test.
Which test to use? This depends upon a number of factors:
1) disease setting – reference hospital or primary healthcare facility
2) available technical skills – fully qualified doctor and/or health technician
3) availability of reagents/test kits/storage facilities in the country concerned.
-
Indirect diagnosis – current use When in a remote settings and primary health care facilities, the most accessible diagnostic is “a proxy”. The most widely used test is the rK39 Rapid Diagnostic Test, which uses a dipstick format to sample blood or serum for the presence of anti-leishmanial antibodies (see Step 2.4). Also used, but in slightly more sophisticated settings, is the Direct Agglutination Test (DAT) which also detects anti-leishmanial antibodies in whole blood (see Step 2.5). Both of these methods are used to guide the decision whether to proceed with an invasive and somewhat risky, confirmatory test.
-
Parasitology Parasitology is used as a term for the detection of Leishmania parasites (amastigote stage) in human biopsy samples. Aspirates from the spleen, bone marrow or lymph nodes for suspected VL and skin biopsy samples for suspected PKDL, are smeared onto glass slides, fixed and then stained and examined under a microscope.
Step 2.6 covers this method. Parasitological examinations allow for the detection of VL in individuals who may present with typical symptoms but test negative in serological tests (e.g. rk39, DAT negative, particularly for immunocompromised individuals). They can also allow the detection of relapse cases and be used as a test-of-cure. A splenic aspiration is more sensitive than alternative bone marrow or lymph node aspirations, but the procedure can be risky and contraindications must be considered.
-
Other methods There are a number of other non-invasive methods to confirm VL diagnosis which use either antibody detection or antigen /parasite detection. Some are new variations of the dipstick test which improve upon the sensitivity in different endemic settings, some are no longer used whilst others require special and expensive reagents, resources and skills that are not always readily available for routine work.
-
New RDTs: rK16, rK18, rK26 or rK28 – developed for diagnosis of VL in HIV patients, PKDL and monitoring of cure
-
ELISA: Same principle as RDT – was developed into the rK39 dipstick
-
IFAT: Antibody detection. Not routinely used any more
-
KAtex: Antigen detection in urine. Poor specificity and tricky to use.
-
LST: Leishmanin skin test – not sensitive enough for VL in an endemic setting[2]
-
Molecular methods. PCR, RT-PCR, nucleic acid sequence-based amplification and LAMP[3] Diagnosis and speciation from blood, minaturisation of PCR reaction to hand-held device. IgG subclasses to monitor relapse[4]
-
Diagnostic pathway
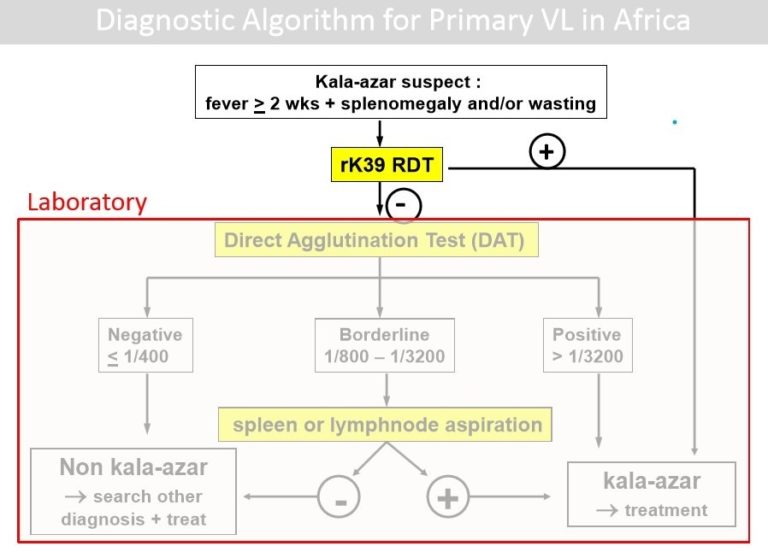
The case definition of VL should be fulfilled before embarking on confirmatory diagnosis. The patient presenting should have had a fever of more than 2 weeks duration, marked weight loss and splenomegaly and/or lymphadenopathy. In the majority of endemic settings the initial point-of-care test is the rK39 dipstick (Step 2.4). If this is positive a splenic biopsy is usually carried out to confirm the presence of Leishmania amastigotes. In some settings, e.g. East Africa, the rK39 test does not deliver a conclusive result and so a DAT test may be performed (Step 2.5). If this is positive (+), a confirmatory splenic biopsy is then indicated to confirm VL. Below you can look at an example of an algorithm used for VL diagnosis.
Example of a diagnostic algorithm for suspected primary VL (courtesy of MSF) [5]
Differential Diagnosis
As highlighted at the end of Step 2.2, there are other infections which have similar symptoms to visceral leishmaniasis. It is important to follow the case definition and to be aware of what may be present in the population. The rK39 test for example, will not work in some cases and this could be indicative of other disease. Given the expense and side effects of VL chemotherapy, it is important to be able rule out VL treatment.
Control and Elimination of Visceral Leishmaniasis


Control and Elimination of Visceral Leishmaniasis
Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.




