
Antimicrobial Stewardship in low and middle income countries
This case is from South Africa but the issues can affect all low and middle income countries (LMIC).
The case occurred in a Tertiary academic hospital. The hospital had an antimicrobial stewardship programme based around a restricted formulary and antimicrobial stewardship guidelines provided to all staff.
Background to the case
A graph showing the resistance rates of S. aureus 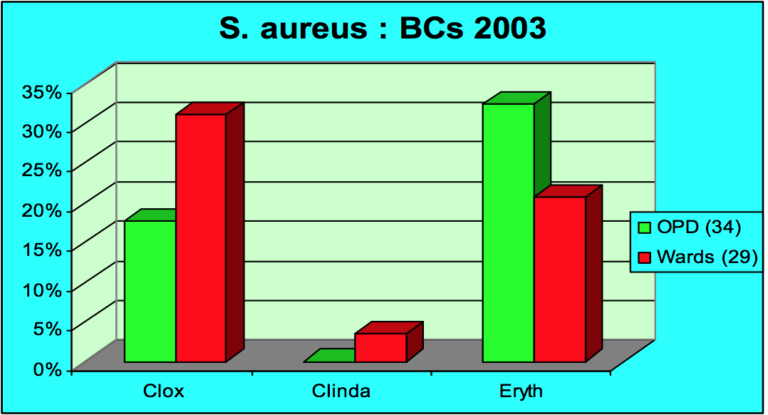 Clox = Cloxacillin. Clinda = Clindamycin. Eryth = Erythromycin. OPD = outpatient department.
Clox = Cloxacillin. Clinda = Clindamycin. Eryth = Erythromycin. OPD = outpatient department.
S. Aureus resistance rates in the hospital at this time in the outpatient setting were approx. 15-16% of S. Aureus isolates with MRSA; in general wards this was around about 30%. The high rates of MRSA in the outpatient setting were probably a reflection of patients who start to return to outpatients for follow up. So we don’t have a true breakdown of how many of those Outpatient Department patients had true community acquired MRSA. However, MRSA rates are sitting at about 30%.
At the time of this case restricted antimicrobials requiring approval before being given to patients included:
• Acyclovir: intravenous
• Cefepime
• Ceftriaxone
• Ciprofloxacin: oral & intravenous
• Clindamycin: oral & intravenous
• Fluconazole: intravenous
• Imipenem
• Meropenem
• Piperacillin/tazobactam
• Vancomycin
The straight forward restricted policy procedure: 
The physician would see the patient whom he thought required a restricted antibiotic. They would then phone either the on call microbiologist or infectious disease clinician, who would act as the “gate keeper/policemen”. They discuss the case and if the restricted agent was thought to be appropriate because of clinical presentation or microbiological results, then the pharmacy would be contacted and the agent approved for the patient. The microbiology lab and ID department provided a 24hr on call service for this purpose and restricted agents were available after hours for emergency patients too.
The patient case
- Blood culture taken – Gram positive cocci in clusters
- Blood culture collected from a 23-year-old male
- Involved in a motor vehicle accident
- Suffered a fractured femur (plus other injuries) – external fixator
- In hospital 6 days
- Became pyrexial on day 4 post-surgery – no clear source of infection, but concern about soft tissue infection.
- Commenced on IV cloxacillin plus gentamicin
The problem with this case
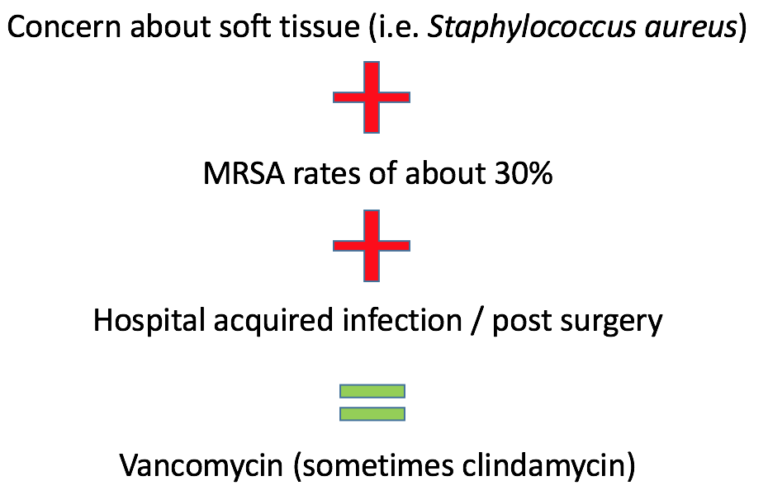
If you look at the clinical presentation of a soft tissue infection where S. Aureus is the most likely antigen, institutional MRSA rates are roughly 30%. The patient had been in hospital for 4 days before becoming septic (hospital acquired infection) and post surgery. The local guidelines at that stage called for the use of vancomycin empirically if suspecting such a hospital acquired infection. Occasionally clindamycin is used as an alternative. This patient had not received vancomycin but cloxacillin.
So why was the wrong drug used in this case?
Lack of knowledge?
- Guidelines were readily available to all staff; susceptibility data was not always readily available (a weakness from the laboratory service).
Lack of drug?
- The drug was available in hospital pharmacy
Lack of time? This seems to have been the main issue:
- “easier to write up an unrestricted agent than phone microbiology / infectious disease”
This illustrates one of the big challenges with antimicrobial stewardship = ACCESS VS EXCESS.
Clinicians perception of antimicrobial stewardship is that it is trying to cut down and reduce access to antimicrobials. This is a part of stewardship but if patients don’t get the right antibiotics they will not do as well as they should. So we know the use of appropriate agents at the right time improves clinical outcomes and we have good clinical data to support this.
On the other hand the inappropriate and over use of broad spectrum antimicrobials is linked to collateral damage:
The main aim of any prescribing should be to improve clinical outcomes.
Causes of limited access
So this patient received an inappropriate antibiotic. This table is based on a publication by “The Access to Medicine Foundation” looking at the causes of limited access to drugs.
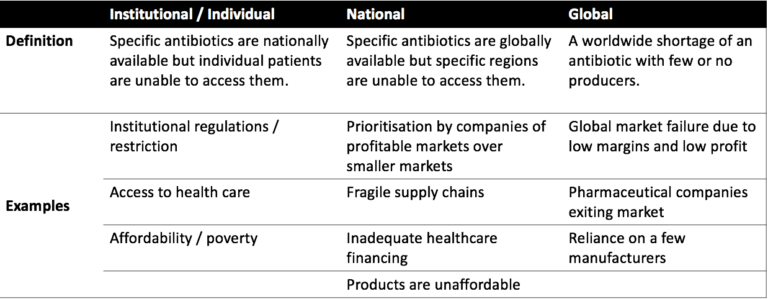
In LMIC access to healthcare can being restricted because of lack of facilities and the affordability of care and medicines. What you are prescribed can be directly linked with what you can afford to buy.
When you are setting up any stewardship programme, whether at institutional or national level, one needs to bear in mind that the right patients get the right antibiotic when they need them.
So what happened in this case?
The blood culture was isolated to staphylococcus.
The patient responded well. He was afebrile at the time the results were phoned in. The antibiotics were not changed. The evidence for infection had been soft – fever, some swelling at pin-sites. The question is did he even need an antibiotic?
So we need to focus on access to antimicrobials and ensuring they are available to the right patients when they need them.


Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.




