
Surveillance
Along with antibiograms, there are a number of ways surveillance plays a vital role in AMS. But first…
What is surveillance?
WHO defines surveillance as “the continuous, systematic collection, analysis and interpretation of health-related data.” Surveillance can help inform policies and infection prevention and control responses.
Surveillance can also be specific to AMS and is an important aspect of tackling AMR. This involves the collection, analysis, and interpretation of antimicrobial resistance or antimicrobial use data. This data should be continuously collected, to best inform guidelines and AMS policy.
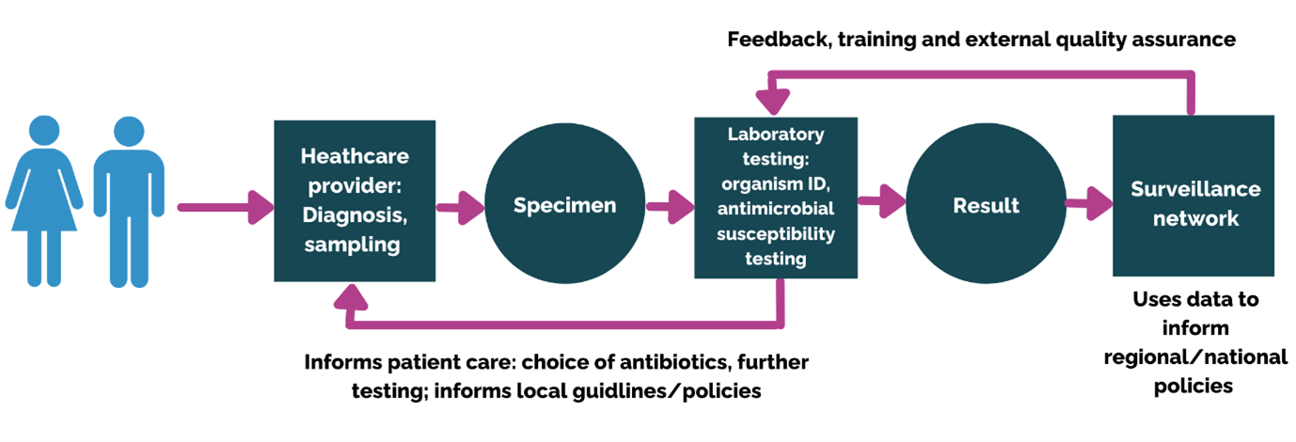
Surveillance requires a readily available source of data. For AMS, the core data needs to be generated by microbiology laboratories, patient medical notes, prescribing charts, and hospital pharmacy stock systems. This data needs to be provided promptly to inform decision making and action.
The image below shows surveillance in action, highlighting how it works to support AMR.

Click here to see a larger version of this image.
The kinds of data that AMR surveillance can collect at a hospital level is summarised in the figure below.

To support surveillance, certain tools such as antibiograms (discussed in the previous step) can be used. An antibiogram allows the monitoring of facility and/or community-specific antimicrobial resistance trends. Antibiograms guide the development of antimicrobial policies by directly tackling the problem of AMR in a systemic manner. In addition, antibiograms can help understand the local prevalence of the most common organisms isolated from different specimens and their antibiotic susceptibilities.
Why is surveillance important?
Surveillance is an important part of ASPs, both surveillance of resistance and surveillance of antimicrobial use. Surveillance of antimicrobial resistance (AMR) tracks changes in microbial populations, permits the early detection of resistant strains and supports the prompt notification and investigation of outbreaks. In addition, surveillance findings are needed to inform clinical therapy decisions, guide policy recommendations, and assess the impact of resistance containment interventions. The image below shows how AMR surveillance can improve health outcomes.

The World Health Organization launched the Global Antimicrobial Resistance Surveillance system (GLASS), a pillar of the global action plan on AMR and surveillance, to address the issue of most countries not having good quality AMR data. WHO wanted to measure the regional AMR burden to generate quality data, and they supported countries in establishing effective national AMR surveillance. GLASS is used for clinical specimens sent routinely for microbiological examinations for pathogens to test their susceptibility to certain antibiotics. GLASS is a case-based surveillance system, e.g. it includes the demographic features of patients, as well as stratifying community-acquired infection (CAI), and hospital-acquired infection (HAI).
Click here to see the Global Antimicrobial Resistance Surveillance System, and here to read more about GLASS and antimicrobial consumption surveillance.
Surveillance is the foundation for assessing the spread of AMR and informing and monitoring the impact of local, national, and global strategies. GLASS provides surveillance based on laboratory data to a system that includes epidemiological, clinical, and population-level data.
GLASS also now incorporates monitoring the use of antimicrobial medicines and also AMR in food and the environment. It provides a standardised approach to collecting, analysing, interpreting and sharing data in many countries whilst actively supporting the capacity, monitoring, and building the status of new and existing surveillance systems.
Ten key attributes should be considered when determining if a surveillance system will be effective.
- Usefulness: How useful is the system in accomplishing its objectives?
- Data quality: How complete and accurate are the data fields in the reports received by the system?
- Timeliness: How quickly are reports received? Timeliness might be necessary for certain conditions but less critical for others. You might need to report one disease immediately to implement contact avoidance and prevention measures. A longer delay in reporting is acceptable with other conditions, such as obesity.
- Flexibility: How quickly the system can adapt to changes.
- Simplicity: Is the system easy to operate?
- Stability: Does the surveillance system work well, or does it break down often?
- Sensitivity: How well does the system capture the intended cases. Does it capture 60% of the cases or 80%? If you have a system that only captures 60%, but 80% is needed, it might not be effective enough for that condition or situation.
- Predictive value positive: How many of the reported cases are actual cases that meet the criteria for what we call a case — that is, how many reported cases meet the case definition?
- Representativeness: How well the system represents the population under consideration. Does it identify events only among certain groups, or does it accurately capture events across the target population?
- Acceptability: How willing are the system users to participate in the surveillance efforts actively and report their data.
The Fleming Fund have produced an excellent course that dives deeper into the topic of AMR surveillance. Click here to learn more!
Surveillance of antibiotic use
Surveillance of antibiotic use is a cornerstone of any antimicrobial stewardship programme, and surveillance can help to improve the quality of prescribing. There are two main ways in which antibiotic use can be measured:
Quantitatively: This approach uses data from hospital pharmacy stock management systems showing information about antibiotics sent to wards and departments, which in the absence of electronic prescribing systems can be used as a proxy for antibiotics administered to patients.
Qualitatively: A qualitative approach is required to provide information on which patients are being given which antibiotics, their indication, which antibiotics are being used for treating particular infections and whether the antibiotics prescribed follow local prescribing guidelines. This type of qualitative information can be collected in a structured way using Point Prevalence Surveys (PPS), which can then be fed back to prescribers to define areas for improvement.
To read more about surveillance of antibiotic use, have a look at the BSAC PPS course, right here on FutureLearn!
How to set up an Antimicrobial Stewardship Programme


How to set up an Antimicrobial Stewardship Programme
Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.





{kind=link}