
How to engage patient and public in research to tackle AMR
In this presentation, Dr Enrique Castro-Sanchez, Lead Academic Research Nurse and Honorary Consultant Nurse in Communication and Patient Engagement at the NIHR Health Protection Research Unit for Healthcare Associated Infection and Antimicrobial Resistance at Imperial College London, highlights a number of key considerations when trying to engage with patients and members of the public in research to tackle AMR.
He provides evidence-based insights into the broader aspects of engaging with patients and the public, including their perceived role at a national level, the language we use to discuss antibiotic use, the level of health literacy in different groups, and other social determinants which may influence their understanding and decisions around antibiotic use.
The video covers the following topics:
- How can we involve patients in the AMR debate?
- Citizens roles in AMS interventions as defined by national policies
- The language of AMR needs consideration
- Health literacy in AMS and infection
- The role of social determinants in enabling patient participation in AMS
Some of the options that enable us to support the participation of citizens/patients in AMS
- Offering education to patients and citizens about antimicrobial resistance and appropriate use of antibiotics
- Ensuring that patients have got adequate self-efficacy skills to prevent infections – for example adopting behaviours such as vaccination or hand hygiene
- Facilitate the participation of patients and citizens in antimicrobial resistance policies
- Collaborating with patient and citizen groups to address wider factors that encourage the development of infections
 Click here to take a closer look
Click here to take a closer look
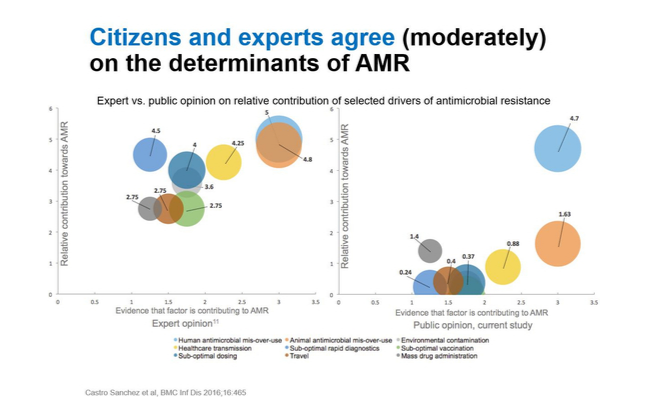
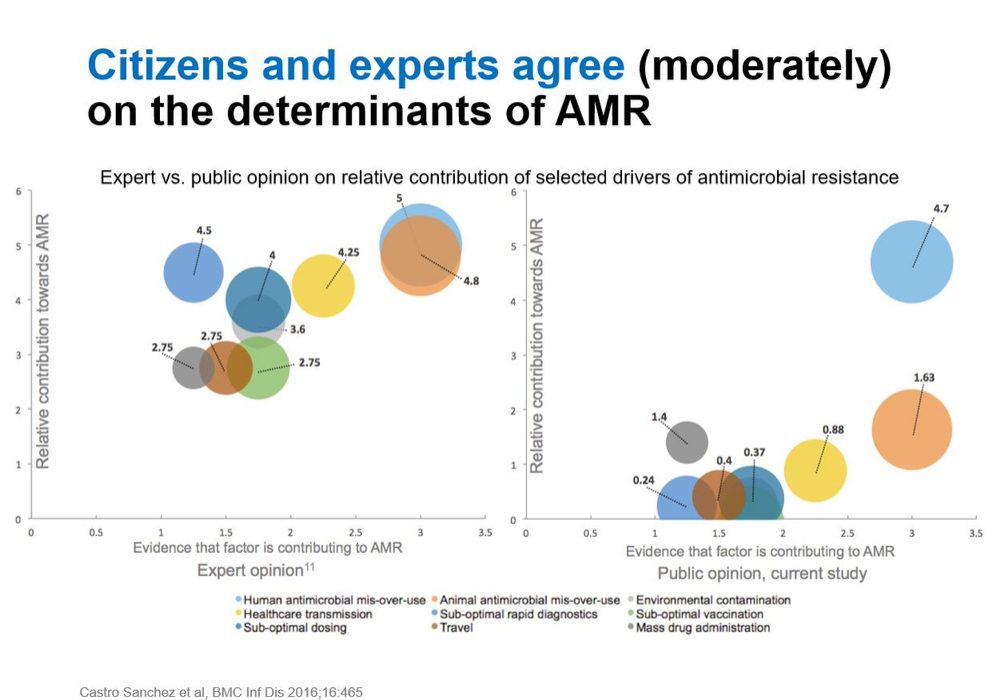
Campaigns have an impact in ensuring the views of citizens and experts regarding determinants of antimicrobial resistance are aligned. The image above shows research suggesting the public attribute development of resistance to a single factor – mainly misuse/overuse of antimicrobials in human health. This is shown on the right hand side.
The left hand side shows the factors experts feel are most important in development of resistance. There is a dramatic contrast, as experts appear to hold several factors at the same level of importance.
These findings are important as they allow us to design campaigns focused on citizens, which are tailored to the views citizens have.
Mapping health literacy – infection studies
Under see also you will find links to studies exploring the relationship between health literacy and antibiotic use.
There are some areas where no health literacy studies have been conducted:
- Linking health literacy and hand hygiene
- Chlamydia
- Herpes
- Malaria
- Leprosy
- Dengue
- Leishmaniasis
- Tuberculosis
- Clostridium Giardiasis
- Campylobacter Cholera
- Escherichia coli
What interventions can be carried out to address health literacy deficits?
One example could be aiming to improve the existing typical patient information on websites: often this can be not interestingly displayed, and it is static and impersonal to the patient.
A solution to this could be the development of apps which offer information relating to patient safety. For example, there may be videos which show users how to conduct proper hand hygiene, podcasts which teach patients how to prepare for surgery, and maps which show the location of their appointments.
Under see also you can find additional reading for this step.
Please find a pdf of the PowerPoint slides in the downloads section below.
In the comments below please let us know:
- What are some options for the participation of citizens/patients in AMS in your setting?
Tackling Antimicrobial Resistance: A Social Science Approach


Tackling Antimicrobial Resistance: A Social Science Approach
Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.



{kind=link}