
How do Fungi cause disease? – Part 1

It is important to understand how fungi cause disease in order to know how to prevent the development of infection and to control its source when infection has already developed. Infection prevention and source control are key factors in antimicrobial stewardship.
Most of the 500 species of fungi that can cause disease in humans mainly do so in susceptible hosts, and are thus are classified as opportunistic pathogens. There are, however, some 100 species of fungi that can cause disease in healthy individuals, and are classified as primary pathogens. This classification is, however, over-simplified as most fungal pathogens can cause a disseminated infection also in immunocompetent individuals if the infective dose is high enough (e.g. by inhalation of high levels of spores or gut perforation due to trauma).
 Fusarium sp. on dextrose agar plate
Fusarium sp. on dextrose agar plate  E. floccosum on agar plate
E. floccosum on agar plate
The source of endogenous fungal infections is the patient’s own gut flora whereas the source of exogenous fungal infections is in the environment.
The key factors that define the outcome of exposure to any micro-organism are infectivity, pathogenicity and virulence.
- Infectivity is an organism’s ability to infect a host. Exposure may lead to carriage (colonisation) or symptomatic disease, and be long lasting (chronic) or self-resolving and transient.
- Pathogenicity is the ability of an organism to cause disease (harm to the host) which depends on host-pathogen interactions such as specificity to species (human pathogen) and host’s immunological status (opportunistic vs primary pathogen).
- Virulence is the degree of pathology caused by the organism. This is reflected by the ability of the pathogen to multiply within the host and is mediated by virulence factors.
The infectivity, pathogenicity and virulence of fungal pathogens varies significantly between species:
- Some dermatophytes (e.g. those causing athlete’s foot) are very infectious but exposure does not always lead to the development of symptomatic infection. If infection does develop, this is normally limited to the skin and the affected site. However, deeper and disseminated infections are seen in severely immunocompromised individuals.
- Candida species are common colonisers of the mouth, GI tract, genital areas and moist areas of the skin whilst human to human transmission is rare and limited to neonates and severely immunocompromised individuals. If the amount of Candida exceeds the tolerance of the underlying skin or mucosa (due to favourable environmental conditions or weak local or systemic immune responses) a localised superficial infection may occur. On the other hand, Candida can survive in the blood stream and cause systemic infection if it gains access to it through vascular lines or damaged GI tract mucosa. However, this is mainly seen in critically ill or otherwise immunocompromised patients.
- Spores of Aspergillus and other environmental moulds are commonly present in outdoor and indoor air. We all inhale thousands of spores every day but our airways have various mechanisms to clear them without significant inflammation or damage. In severely immunocompromised individuals the exposure can lead to the development of infection, which typically is invasive with high mortality. On the other hand, some immunocompetent individuals develop hypersensitivity to moulds which can exacerbate their asthma.
Immunocompromised patients are not only at risk for more severe infections but also recurrent superficial infections caused by various opportunistic pathogens. Recurrent fungal infections may be a sign of an immunodeficiency which should be kept in mind when managing such infections.
Route and site of infection varies between the fungi and the immune status of the host. Fungi can cause disease through:
- Replication of the fungus (fungal cells can invade tissues and disrupt their function)
- Immune response (by immune cells or antibodies)
- Competitive metabolism (consuming energy and nutrients intended for the host)
- Toxic metabolites (for example Candida species can produce acetaldehyde, a carcinogenic substance, during metabolism)
Compared to bacteria, less is known about the mechanisms by which fungi cause disease.
Superficial mycoses
Superficial fungal infections affect the outer layers of the skin, the nail, hair or mucous membranes. They can also act as a source of deeper infections in immunocompromised patients, and the skin lesions can act as a portal of entry for bacterial pathogens. Therefore, it is important to look for and manage these infections in all hospitalised patients.
 Superficial fungal infection of trichophyton tonsurans
Superficial fungal infection of trichophyton tonsurans 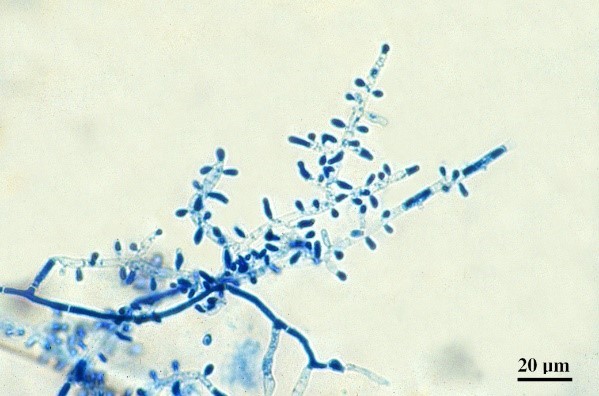 Trichophyton tonsurans under the microscope
Trichophyton tonsurans under the microscope
Dermatophytes are a group of fungi that live on the skin, nails and hair. They pass from host to host and rarely cause significant disease. Most dermatophytes can survive in the built environment (public bathing places, sports facilities) and this contributes to host to host transmission. The host inflammatory responses to human dermatophytes is usually minimal but can be more severe in case of zoonotic (species normally causing disease in animals) infections (infection contracted e.g. from pets).
Candida, most commonly Candida albicans, is a common human commensal. It lives on the mucosae, moist areas of the skin and in the gastrointestinal tract. If host factors change (environmental conditions, immune responses) or the amount of Candida exceeds the tolerance of the underlying mucosa (poor dental hygiene), then resident Candida can result in an infection of the mucosal surfaces (thrush). The source for thrush, in most cases, is patient’s own colonisation. Human to human transmission is mainly seen in neonates (mother to child). Thrush is not sexually transmitted. Cutaneous Candida infections are mainly seen in patients with immunodeficiencies.
 A patient suffering from cutaneous candidosis
A patient suffering from cutaneous candidosis  A patient suffering from chronic oral candidosis
A patient suffering from chronic oral candidosis


Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.




