
Delivering a mobile outreach DR service
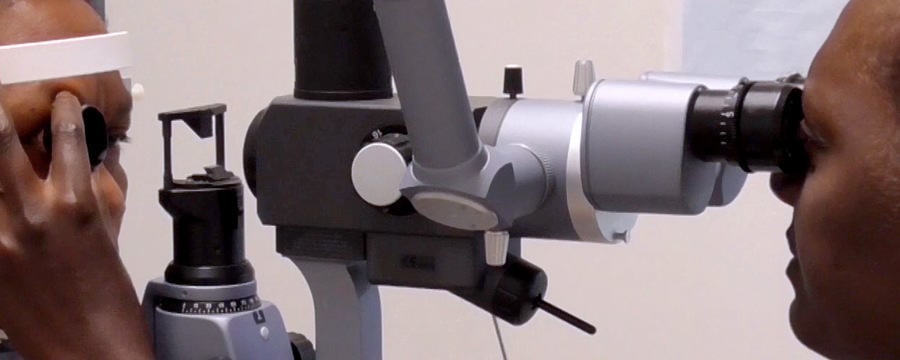
58 year old teacher Dora has come to the mobile DR service because she heard about its scheduled visit at the local health centre. She has recently noticed some vision loss which she initially attributed to getting old and needing glasses. Dora has been on insulin for type 2 diabetes and hydrochlorothiazide for hypertension for 7 years. During this period, she has had multiple emergency admissions to hospital with out of control diabetes. She does not monitor her blood sugars regularly but her last HbA1C test about 6 months ago was 11%.This is Dora’s first eye examination since she was diagnosed with diabetes. She is distressed and worried. She never knew that diabetes could affect her sight. Her vision is found to be 6/60 in both eyes and does not improve with pinhole test. The fundus examination reveals she has severe pre-proliferative diabetic retinopathy and early cataracts.
A mobile diabetic retinopathy (DR) service is a public health strategy to provide targeted screening and other services to people with diabetes who live in different locations. A mobile DR service is essential in many places to maximise available resources and extend the reach of the service.
Key features of a mobile DR service
A mobile DR services needs to:
- Provide a high quality service under all conditions
- Provide a reliable and regular service to gain the support and confidence of local health providers and the population being served
- Monitor data to keep track of the services being provided and the resources needed.
Important considerations for a mobile DR service
Before starting the service it is important to consider at the local level:
- The evidence on the need for DR services in this setting
- The current DR screening practices and guidelines
- The activities to be carried out and outcomes to be achieved
- Which locations to target, and how often
- The local stakeholders that need to be involved
- The values, beliefs and social customs in the target population
- The resources that are needed including funding
- The expectations for return on investment (ROI)
- If there are potential conflicts with existing health services or service regulations
- How will the service be coordinated and monitored
- When the service could be stopped.
In the video on this step, we explore the key components of a mobile DR service and hear from Dr Kibata Githeko, who in 2011 established a DR mobile service in Kenya which he continues to manage today. He shares some of his learning with Dr Nyawira Mwangi from the Kenya Medical Training College.
Key components of a mobile DR service
As you go through this step, reflect on the factors that may affect the implementation and sustainability of a mobile DR service, within your setting or in Ormo (our hypothetical case study). At the planning stage, should we also consider when to stop mobile services at a particular location? If yes, what evidence would you use to guide the decision on when to stop?
Diabetic Eye Disease: Building Capacity To Prevent Blindness

Diabetic Eye Disease: Building Capacity To Prevent Blindness
Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.


