
Definitions of Harm Reduction

As you may have noticed in the previous video, harm reduction is a very broad concept. It is not easy to capture the full concept into one short definition. In fact, it can fills books or, indeed, a fully dedicated E-course.
You can find harm reduction being described as an approach, a ‘way of doing things’, a set of services, or even a mindset, a philosophy or a movement. In this course you will hear speakers talk about different services and structural interventions, primary healthcare, person-centred care, as well as being reflective and critical with a pragmatic mindset, being open-minded, being non-judgemental, adapting to the daily realities… all aiming at improving the social and physical well-being for (often criminalised) individuals and at the benefit of the wider society.
It is important to realise that the diversity of descriptions does not mean that there is disagreement on the fundamental principles of what harm reduction stands for. This course will provide you with many elements and perspectives to describe harm reduction. Also in the next section you will find some components of often-used definition and references, but this course will not provide you with one fixed singular definition of harm reduction. The aim is that by the end of the course you should have a deep understanding of harm reduction and, more importantly, you should find yourself capable of describing harm reduction in your own words.
Definitions
Many definitions or descriptions of Harm Reduction often start by referring to both public health and human rights (or social justice). You will find this back in how this course is structured as the following two topics will look into pubic health and human rights. Furthermore, an undeniably indispensable core-component of harm reduction is the role of the community. You will see this reflected in the fourth topic of this course; the community at the heart of the response.
You will find most definitions providing one or two key-phrases, with an accompanying text to provide a broader description and completing notions. We encourage you to use the links and read the full definitions, as it provides more references and additional notions.
You can find one widely used definition on the website of Harm Reduction International, an organisation which advocates for harm reduction worldwide and which monitors the scale of global harm reduction efforts (and a steering committee members of this course); “Harm reduction refers to policies, programmes and practices that aim to minimise negative health, social and legal impacts associated with drug use, drug policies and drug laws”.
You can find an almost indentical definition (but with a focus on HIV) here on the website of the European office of WHO; “Harm reduction is a set of policies, programmes, services and actions that aim to reduce the harm to individuals, communities and society related to drugs, including HIV infection. Harm reduction is key in the prevention of HIV infection among people who inject drugs (PWIDs) and their sexual partners.”
The Global Commission on Drug Policy includes the notion of self-determination in one of their 10-year anniversary report “Harm reduction is a practice and set of policies premised on respecting personal autonomy while reducing the social and health consequences of problematic drug use.”
For optional further reading; in the download section you will find a document developped by Mainline, AFEW (Aids Foundation East & West), Bridging the Gaps and INPUD (International Network of People Using Drugs) with 10 key points decribing Harm Reduction. (or follow this link)
Principles
The definition of harm reduction offered by Harm Reduction Coalition here emphasises that this is an approach that is a “movement for social justice built on a belief in, and respect for, the rights of people who use drugs.”
Harm Reduction International adds that it focuses on “positive change” by working with people “without judgement, coercion, discrimination” and without requirement that they “stop using drugs as a precondition of support”.
Let’s take some of these key principles we’ve seen so far as a starting point. Harm reduction is:
- Pragmatic
- Non-judgemental
- Empowering
The next video will diver deeper into some of these and other core principles of a harm reduction approach. Taken together so far, it is clear that harm reduction is not just about prevention. It is an approach to WORKING WITH people who use drugs that sees social justice at its heart, of which health and well-being are integral parts.
Harm Reduction International elaborates the principles of harm reduction in the following ways:
- Respecting the rights of people who use drugs
- A commitment to evidence
- A commitment to social justice and collaborating with networks of people who use drugs
- The avoidance of stigma
These are helpfull notions, with some examples of what these principles mean;
The use of drugs does not mean people forfeit their human rights – they remain entitled to the right to life, to the highest attainable standard of health, to social services, to privacy, to freedom from arbitrary detention and to freedom from cruel, inhuman and degrading treatment, among others.
Harm reduction policies and practices are informed by a strong body of evidence that shows interventions to be practical, feasible, effective, safe and cost-effective in diverse social, cultural and economic settings.
Harm reduction is rooted in a commitment to addressing discrimination and ensuring that nobody is excluded from the health and social services they may need because of their drug use, their race, their gender, their gender identity, their sexual orientation, their choice of work, or their economic status.
Harm reduction practitioners accept people who use drugs as they are and are committed to meeting them “where they are” in their lives without judgement.
Practices
- Keeping people alive and encouraging positive change in their lives; and
- Reducing the harms of drug laws and policy
The criminalisation of people who use drugs; abusive and corrupt policing practices; the denial of life-saving medical care and harm reduction services; restrictions on possession of injecting paraphernalia; forced urine testing and detention in the name of rehabilitation; and, discrimination based on drug use, class, race, and gender.
The environments affecting drug use and drug harms are, however, broader than policy and law. As we will trace through the various steps in this course, the environment affects drug harms also through the physical environment, the social environment and the economic environment, in addition to the policy environment. In Step 1.15 we discuss ideas of ‘risk environment’, and how harm reduction interventions seek to turn these into ‘enabling environments’ for health.
Harm reduction can therefore mean many different and intersecting things in practice. It encompasses interventions aiming for individual, community, social, and structural change. Here is a list of some of the interventions of harm reduction, many of which you will hear experts in this course talking about:
- needle and syringe programmes
- opioid assisted therapy and drug treatment
- HIV and viral hepatitis prevention and treatment
- overdose prevention and reversal
- drug checking
- drug consumption facilities
- psychosocial support
- information on safer drug use
- peer intervention and drug user organising
- stigma reduction
- housing and employment initiatives
- drug policy and law reform
- human rights advocacy
While the focus of harm reduction intervention, by definition, is not a goal to achieve abstinence from drugs, the package of interventions making-up harm reduction can also include different forms of drug treatment, including helping people to reduce or stop their drug use when they wish to.
Structural interventions
What we have seen in the harm reduction field over the past two decades is a growing shift towards recognising the importance of social and structural interventions alongside those targeting individuals and communities. Drug policy reform is one element of structural intervention seeking to create environments that are enabling of health for people who use drugs.
The World Health Organization, despite being a public health agency, recognises the need for looking beyond the health sector and addressing critical enablers because “HIV epidemics, particularly among key populations, continue to be fuelled by stigma and discrimination, gender inequality, violence, lack of community empowerment, violations of human rights, and laws and policies criminalizing drug use and diverse forms of gender identity and sexuality. These socio-structural factors limit access to HIV services, constrain how these services are delivered and diminish their effectiveness.“
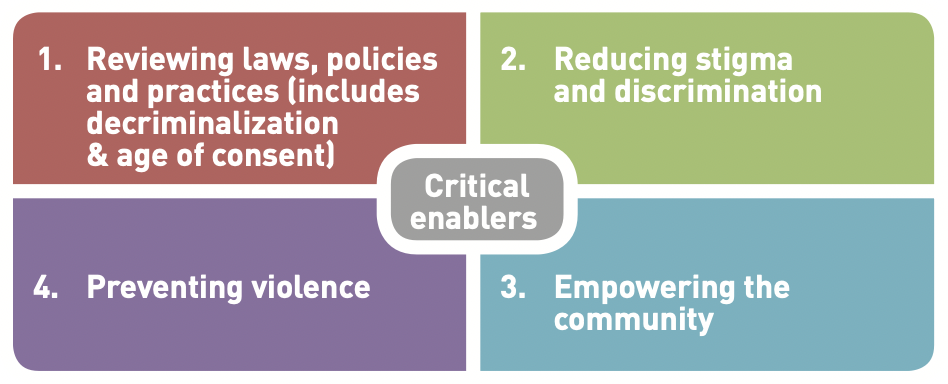
In the WHO Consolidated guidelines on HIV prevention, diagnosis, treatment and care for key populations (see here). The WHO defines critical enablers here as “strategies, activities and approaches that aim to improve the accessibility, acceptability, uptake, equitable coverage, quality, effectiveness and efficiency of HIV interventions and services” and defines 4 areas of critical enablers.
Importantly, in the same guideline, the WHO officially recommends that “Countries should work toward decriminalization of behaviours such as drug use/ injecting, sex work, same-sex activity and nonconforming gender identities, and toward elimination of the unjust application of civil law and regulations against people who use/inject drugs, sex workers, men who have sex with men and transgender people”
What do you think of this as guidance? Do you agree with it? Thinking of your own setting, how feasible is such a policy change, and how would it advocate for it?
Interventions advocating decriminalisation are rooted in evidence, both evidence of the harm that drug policies that criminalise can do, and evidence of the harm reduction that removing or reforming these policies can bring. We discuss this evidence in more detail in week 2, in Step 2.8.
Nothing about us, without us
Last, but perhaps most importantly, harm reduction fundamentally stands for community involvement and aims at empowering people who use drugs to represent their own community. There is an obvious paradox in giving a voice to people, that in many places, are considered to be criminals. Speaking up as a person who uses drugs can lead to a lot of problems. This is a complex but essential component of harm reduction.
The fourth week will look more into the role of community-based and community-led harm reduction and expands on two component of community mobilisation; peer work and self-organisation.
Nothing new
Lastly, we want to indicate that harm reduction in the drugs field has a long history. It can be traced back to the prescription of heroin and morphine to people dependent on opioids in the UK in the 1920s, and to the introduction of methadone maintenance in the USA in the 1960s. In 1974, the World Health Organization (WHO) recommended policies of harm reduction to “prevent or reduce the severity of problems associated with the non-medical use of dependence-producing drugs”, noting that this goal is at once “broader, more specific” as well as “more realistic” than the prevention of non-medical use per se in many countries.
Harm reduction also connects with shifts in public health more generally. By the 1980s, the ‘new’ public health movement, endorsed by the World Health Organization, had adopted a vision of public health beyond narrowly defined biomedical understandings that re-defined health as well-being more generally, and which saw harm as a product of the social and policy environment (WHO, 1986). This gave much greater emphasis to community-based risk reduction, including through community involvement, and less emphasis on health service based treatment alone. Harm reduction is an exemplar ‘public health’ intervention.


Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.




