
Types of AMS interventions
In this step, we will explore the types of AMS interventions available.
AMS interventions are the activities or structures and processes that are put into place to change and optimize antibiotic prescribing practice. They exemplify the core work of antimicrobial stewardship teams.
So far in this course, we have explored the need for AMS and, in the last step, briefly mentioned some potential ”low hanging fruit “ AMS interventions. In this step, we will broadly categorise the four different types of AMS interventions and, within each category, give examples of different types of interventions and explore the “core” activities in a little bit more detail.
Core or key evidence‐based stewardship interventions include empirical treatment according to local or national guidelines, de‐escalation of treatment, parenteral‐to‐oral switch, therapeutic drug monitoring, and restricted antimicrobial lists demonstrate benefits in terms of clinical outcome, adverse events, treatment costs, and antibiotic resistance rates. These benefits are outlined in an excellent systematic review and meta-analysis.
Why are AMS interventions important?
Throughout this course, we shared details from the valuable 2017 Cochrane review. The review is incredibly useful in highlighting the importance of AMS interventions for hospital inpatients. The review demonstrates that enabling and restrictive interventions are associated with:
- A 15% increase in compliance with desired practice (such as increased compliance with antibiotic policies).
- A 1.95‐day decrease in the duration of antibiotic treatment.
- A 1.12‐day decrease in inpatient length of stay.
- Without compromising patient safety (without an increase in mortality).
As mentioned previously, one limitation of the Cochrane review was the lack of high-quality studies from hospitals in LMIC settings. This was addressed in another systematic review focused on LMICs. Whereas this review generally showed the positive impact of the studies conducted in this setting, it confirmed that good quality studies were scarce to allow strong recommendations to be made. Despite this, there is broad acceptance that applying the core range of AMS activities in the LMIC setting is broadly beneficial.
Categories of AMS interventions
AMS interventions can be grouped into four categories as illustrated in the WHO toolkit (table 7, below), which provides a classification of hospital AMS interventions with examples of each. In most circumstances, a blend or mix of these approaches is often called the “bundled” approach.

Click here to see a larger version of this image.
This infographic is also available as a screen-reader compatible PDF.
Another way to categorise AMS interventions is by grouping them into ‘core’ and ‘additional’ interventions. The image below summarises the range of core AMS interventions commonly used and additional ones. The use and value of these interventions depend on the identified priorities within the hospital and the resources available to implement and evaluate the interventions.
Basic AMS interventions
The WHO toolkit also outlines a core set of ‘basic’ interventions, which are more accessible and require fewer resources. These are outlined below.
Integrating AMS interventions into clinical practice
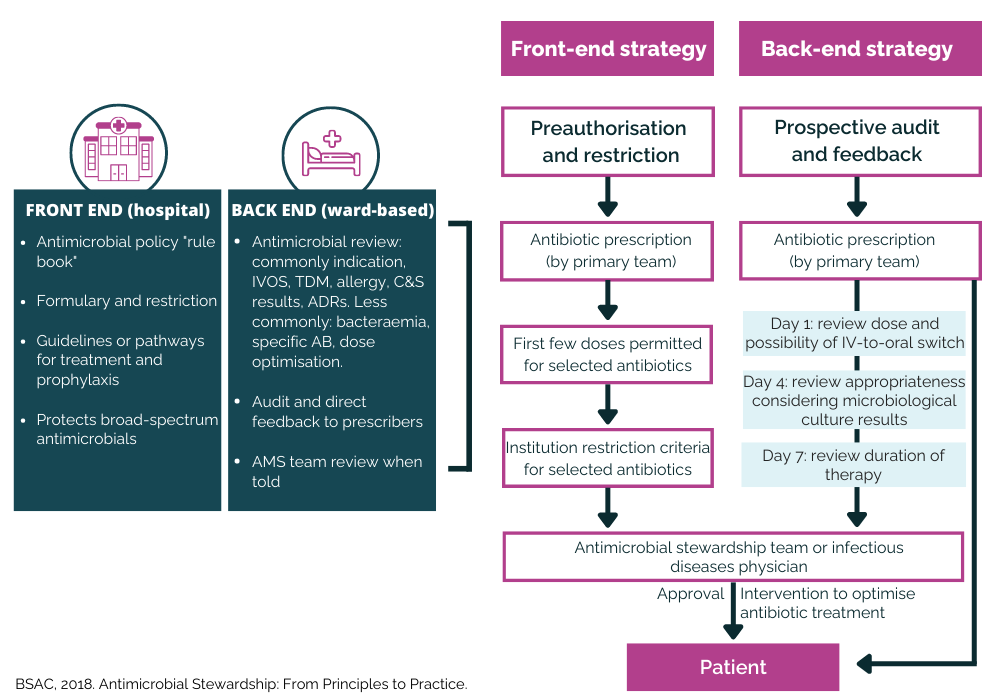
Several experts have created pathways to help understand critical AMS interventions and ensure their integration into everyday practice clinical decision-making. For example, AMS interventions are typically classified as “front end” and “back end”.

Click here to see a larger version of this image.
This infographic is also available as a screen-reader compatible PDF.
Front End
Interventions that target the decision-making process that leads to the prescription and administration of an antibiotic are called “front end” interventions. These happen before or at the time of the prescription and may include:
- Develop empiric syndromic guidelines or pathogen-specific guidelines for prevention and treatment, including antibiotic choice, dose, route, and duration.
- Ensure access to antimicrobials, including essential medicines list antibiotics.
- Restriction through pre-authorisation of certain antibiotics, e.g. use of AWaRe list (Watch and Reserve groups).
- Ensure documentation of indication in notes for all patients who receive antibiotics.
- Ensure medical charts and records are available at all times and in one place.
- Ensure specimen taken for culture and sensitivity testing (requires the availability of laboratory).
- Establish basic laboratory and infection management leadership and expertise (capacity and capability) to support AMS.
Back End
AMS interventions that target the review of a prescribed antibiotic are called “back-end interventions”. These interventions are often associated with feedback to the prescriber following the prescription and administration of antibiotics. They may include:
- Review of indication, antibiotic choice, dose, route and duration of treatment.
- Feedback of prescription review recommendations to prescribers.
- Education of ward-based staff, particularly prescribers.
Evidence suggests that ”back-end” AMS interventions may appear more resource-consuming but are more effective and sustainable in the long term.
A 2017 quasi-experimental, crossover trial study by Tamma PD et al. highlights this. The diagram below shows how they compared antibiotic use by two medical teams assigned to receive initially:
- pre-prescription authorisation (PPA), a front-end AMS intervention, or
- post-prescription review with feedback (PPRF), a back-end AMS intervention.

The study found that PPA increased compliance with policy & guidelines compared to PPRF.
Time series analysis was used to compare days of therapy (DOT), and results showed that PPRF had a more significant impact on decreasing DOT than PPA.
Most hospitals will try to use both interventions but where resources are limited, investing in PPRF may be a more effective option.
In England, a programme called “Start Smart then Focus” has been implemented and this simple and pragmatic care pathway incorporates a range of ”front and back” end stewardship interventions in a manner that is intuitive to clinical prescribing. The diagram below, adapted from the BSAC AMS e-book (page 101) highlights the prescribing principles for empirical antimicrobial therapy from the programme.

Click here to see a larger version of this image.
This infographic is also available as a screen-reader compatible PDF.
The useful example below from the AMS toolkit, provides further details of using audit with feedback.

Click here to see a larger version of this image.
A retrospective audit involves collecting data to evaluate practice in the past and can be useful to evaluate the impact of AMS interventions on antibiotic use. A prospective audit collects real-time data and has the advantage of being able to share feedback on current practice.
Such audits of antibiotic use may be used for several purposes:
- To identify areas for improvement at whole hospital or ward level.
- To evaluate the impact of an intervention.
- To provide regular and structured feedback on the quality and quantity of antibiotic prescribing and use to share with prescribers.
The feedback element is most important as it provides an opportunity for clinical staff to discuss:
- Their prescribing practices.
- Identify priority areas for change.
- Set specific goals for themselves at the facility, department and/or ward level.
Evidence to support AMS interventions
It is essential to clearly understand the evidence base underpinning AMS to help AMS teams become confident in the effectiveness of their approach to antimicrobial stewardship.
Systematic reviews and meta-analyses provide the most robust scientific methods to evaluate the impact of different AMS interventions. It is also essential to understand the impact of these interventions in the context of LMIC settings. Several such analyses have now been published.
We have already discussed some excellent examples in step 1.8, which you can read in more detail by clicking the links below.
- A 2017 study by Baur et al. looked at the impact of AMS on antibiotic-resistant organisms and C. difficile.
- A 2019 study by Nathwani et al. examined the value of hospital AMS programmes.
- A 2018 study by Van Dijck et al. reviewed the impact of AMS interventions in LMICs.
- A 2016 study by Schuts et al. examined the impact of AMS interventions on patient outcomes.
As you can see, there are many different types of AMS interventions. In general, persuasive methods, like a prescription review with audit and feedback, are most effective in the long term. By effectively implementing these interventions by managing and sharing resources, AMS programmes can make steps towards more responsible use of antibiotics.
In our next two steps, we will explore how we can use behaviour change strategies to ensure these interventions are implemented effectively.
How to set up an Antimicrobial Stewardship Programme


How to set up an Antimicrobial Stewardship Programme
Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.





{kind=link}
{kind=link}
{kind=link}
{kind=link}