
Using a realist review to understand complex interventions

In this step, you will be taken through the stages of conducting an example realist review to understand how back-up/delayed prescriptions are used in UK primary care: what works for whom, in what circumstances, in what respects, and how.
The research presented here is part of a grant that is funded by the Economic and Social Research Council (ESRC) as part of The Antimicrobial Resistance Cross Council Initiative which is supported by the seven research councils in partnership with other funders.
Background
A back-up antibiotic prescription (also sometimes called a delayed prescription) is one a prescriber issues to the patient with advice to only use it if symptoms worsen or don’t improve within the expected time. However, despite strong evidence and national guidelines supporting its use, back-up antibiotic prescriptions are not widely offered instead of immediate antibiotics for self-limiting infections such as acute cough, otitis media (middle ear infection), sinusitis, and acute sore throat. A realist review was therefore conducted to answer the question: Why have strategies to issue back-up antibiotic prescriptions not been more widely adopted, and how can we facilitate their uptake?
Approach
Stage 1 – Clarify scope and locate existing theories
In this example realist review, the research team clarified the scope by discussing a number of different considerations such as:
- Only include back-up prescriptions intended for a current self-limiting infection (rather than a potential future infection)
- Focus on understanding why prescribers who want to use back-up prescriptions do not do so as often as they might like (rather than prescribers who do not find this option helpful at all, see figure 1)
- Focus on reducing immediate antibiotic prescribing and minimise potential unintended consequence of increasing back-up prescriptions
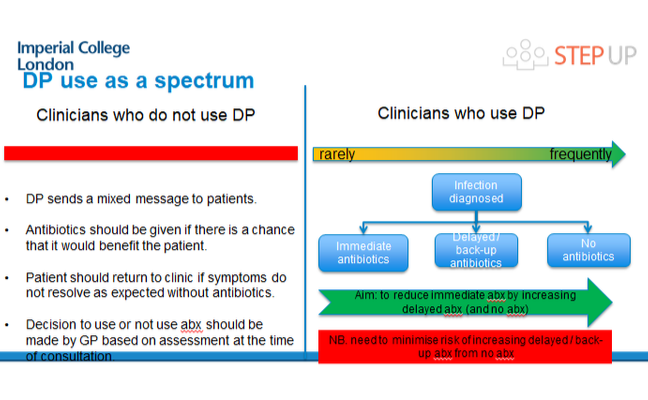 Figure 1 – Delayed prescription use as a spectrum
Figure 1 – Delayed prescription use as a spectrum
Click here to take a closer look
An initial programme theory was then developed based on a preliminary literature search and relevant experience of the team. This basically mapped potential relationships between some of the key barriers and facilitators for using a back-up prescription.
Stage 2 & 3 – Search for evidence, and appraise and select the evidence
To demonstrate the range of evidence that could be included, the example realist review search led to the following evidence being used:
- 76 articles
- Excerpts from interviews with 22 clinical commissioning staff and 19 general practice professionals
- Two stakeholder meetings
- Feedback from 26 citizens
Despite several randomised controlled studies evidencing the effectiveness of using back-up prescription as an alternative strategy to immediate antibiotics, many did not describe how back-up prescriptions were used in sufficient detail. The feedback from interviews, stakeholders and citizens proved invaluable in filling in some of the gaps between research and clinical practice.
Stage 4 & 5 – Extract and organise evidence, and synthesise evidence and draw conclusions
Example early data extraction and coding is illustrated in figures 2 and 3 using the process described in the previous step.
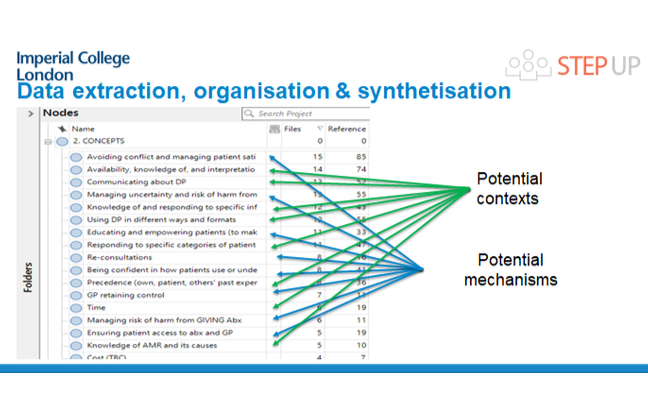
Figure 2 – Potential contexts and mechanisms
Click here to take a closer look
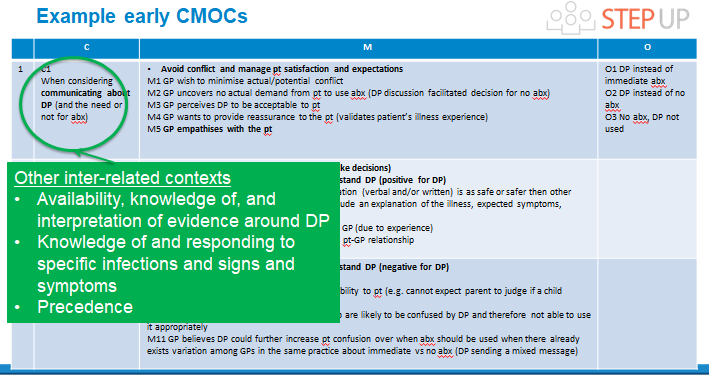
Figure 3 – Example early CMOCs
Click here to take a closer look
The current programme theory shows six interacting constructs that explain how prescribers in primary care shift their decision to prescribe immediate, back-up/delayed, or no antibiotics (figure 4): tolerance of risk of negative consequences; perceived illness severity; diagnostic uncertainty; workload; patient expectations; and patient’s ability to use a back-up/delayed prescription appropriately. Targeting one or more of the identified constructs that is most relevant to the context in which back-up antibiotic prescription is being promoted could lead to positive changes in prescribing behaviour in primary care.
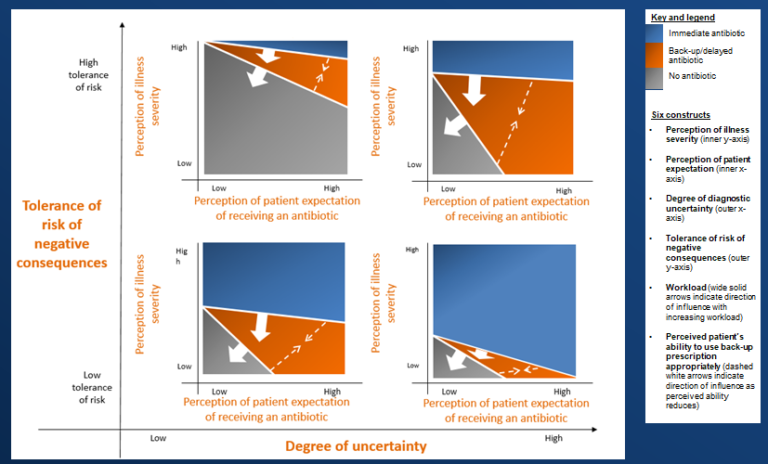
Figure 4 – Decisions to prescribe immediate, delayed, or no antibiotics, and factors which affect this
Click here to take a closer look
Please find optional additional reading on this topic in the see also section below.
Please find a pdf of the images used in this article in the downloads section below.
Tackling Antimicrobial Resistance: A Social Science Approach


Tackling Antimicrobial Resistance: A Social Science Approach
Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.





{kind=link}
{kind=link}
{kind=link}
{kind=link}