
COVID-19 and Sexual and reproductive health

The following is extracted from the article: Riley, et.al. Estimates of the Potential Impact of the COVID-19 Pandemic on Sexual and Reproductive Health In Low- and Middle-Income Countries International Perspectives on Sexual and Reproductive Health 2020; 46: 73-76.
The COVID-19 pandemic is already having adverse effects on the supply chain for contraceptive commodities by disrupting the manufacture of key pharmaceutical components of contraceptive methods or the manufacture of the methods themselves (e.g., condoms), and by delaying transportation of contraceptive commodities. In addition, equipment and staff involved in provision of sexual and reproductive health services may be diverted to fulfil other needs, clinics may close and people may be reluctant to go to health facilities for sexual and reproductive health services. Many governments are restricting people’s movements to stem the spread of the virus, and providers are being forced to suspend some sexual and reproductive health services that are not classified as essential, such as abortion care, thus denying people this time-sensitive and potentially life-saving service. For example, the country lockdowns in Nepal and India have forced clinics operated by Marie Stopes International—the largest provider of family planning services in India outside of the public sector—to close. Without concerted action, access to essential sexual and reproductive health services, and the quality of any care that is provided, will likely decline.
| Disruption in essential SRH care | Impact |
|---|---|
| 10% decline in use of short- and long-acting reversible contraceptives | 48,558,000 additional women with an unmet need for modern contraceptives; 15,401,000 additional unintended pregnancies |
| 10% decline in service coverage of essential pregnancy-related and newborn care | 1,745,000 additional women experiencing major obstetric complications without care; 28,000 additional maternal deaths; 2,591,000 additional newborns experiencing major complications without care; 168,000 additional newborn deaths |
| 10% shift in abortions from safe to unsafe | 3,325,000 additional unsafe abortions; 1000 additional maternal deaths |
Potential annual impacts of a 10% proportional decline in use of sexual and reproductive health care services resulting from COVID-19 related disruptions in 132 low and middle income countries
Previous public health emergencies have shown that the impact of an epidemic on sexual and reproductive health often goes unrecognised, because the effects are often not the direct result of the infection, but instead the indirect consequences of strained health care systems, disruptions in care and redirected resources. Moreover, responses to epidemics further exacerbate gender-based and other health disparities.
Riley el.al. (2020) estimate that a 10% proportional decline in use of short- and long-acting reversible contraceptive methods in LMICs due to reduced access would result in an additional 49 million women with an unmet need for modern contraceptives and an additional 15 million unintended pregnancies over the course of a year.
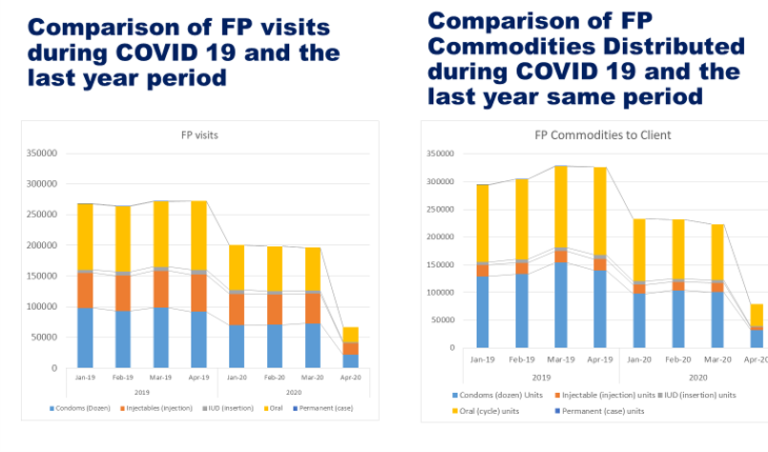
Family planning visits and distribution of family planning commodities between January 2020 and April 2020 in Afghanistan. From Dr. Z Anwari’s webinar (see below).
These model estimates are being confirmed by real data coming from countries as seen by the data presented from Afghanistan by Dr. Z Anwari during a recent webinar sponsored by MOMENTUM. This data shows over 50% decrease in family planning visits and distribution of family planning commodities between January 2020 and April 2020. This far exceeds the estimates predicted by Riley so poses a substantial concern.
Regardless of magnitude or duration, these impacts may be felt most acutely among disadvantaged and neglected groups, including adolescents, those in humanitarian settings, people who identify as LGBTQI, people experiencing gender-based violence, those living with HIV, incarcerated populations, individuals with disabilities and people of lower socioeconomic status.
To avert this potential sexual and reproductive health crisis, LMIC governments and their partners (i.e., donors and nongovernmental organisations) should take swift, decisive action. First, they should define and promote sexual and reproductive health care—including safe abortion, contraceptive services, and maternal and newborn care—as essential. This will allow people to travel for sexual and reproductive health services—even in areas under stay at-home orders or with travel restrictions—without fear of legal consequences. Second, alongside private-sector actors, governments and their partners should strengthen national and regional supply chains—by taking such steps as prepositioning commodities and identifying alternative suppliers—to make sexual and reproductive health medications and supplies more accessible to providers and patients. Third, to improve access to sexual and reproductive health services, they should make contraceptives available without a prescription; decentralise distribution of contraceptives, drugs and other supplies from the national to regional level (to prevent bottlenecks); deliver services at people’s home when possible; and facilitate multi-month dispensing of sexual and reproductive health pharmaceuticals. Fourth, they should adopt innovative models of care, such as tele-health, and prevent diversion of resources and staff away from sexual and reproductive health services. Finally, governments and their partners should address the unique needs of vulnerable and marginalised populations, who often face preexisting barriers to care that are exacerbated during a crisis. These actions will not only mitigate the impact of COVID-19 in the short term, but also provide benefits over the longer term, as innovations are adopted and institutionalised.
Improving the Health of Women, Children and Adolescents: from Evidence to Action


Improving the Health of Women, Children and Adolescents: from Evidence to Action
Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.




