
Donor funding for women’s and children’s health
In 2017, Grollman and colleagues have conducted an analysis of selected donor funding for reproductive, maternal, newborn, and child health worldwide for the period 2003-2013. This work forms part of Countdown to 2015, and is intended to help assess whether donor funding is going to the countries and conditions that most need it, and to promote accountability for change if that is not the case. The 75 Countdown countries were prioritised for support to meet MDG 4 (reduce child mortality) and MDG 5 (improve maternal health), since over 95% of all maternal and child deaths occur in these countries. However only one-third of the prioritised countries met MDG 4 and only 6% achieved MDG 5 1.
What is Official Development Assistance?
Official Development Assistance (ODA) is a record of the amount of international aid received from all donors. This is reported to the Creditor Reporting System of the Organisation for Economic Co-operation and Development (OECD). This aid comes from:
- Bilateral agencies, e.g. a government agency providing aid, including medical aid or disaster relief, and for people in other countries e.g. USAID or UKAID/DFID
- Multilateral agencies, i.e. an organisation obtaining funding from multiple governments and to spend on projects in various countries, e.g. the World Health Organization or the World Bank
- Global Health Initiatives, e.g. Global Fund or GAVI.
Donors not reporting to the CRS, such as China, were not included.
In the analysis, grants given by the Bill & Melinda Gates Foundation from earlier years that are also reported to the CRS were added to ODA values, resulting in what they called ODA+2.
How much ODA is spent on women and children’s health and what are the trends?
Globally, high-level commitments have been made to meet MDG 4 and MDG 5, and these commitments must be matched by funding pledges. Bilateral aid remains the dominant source of funding for reproductive, maternal, newborn and child health (RMNCH).
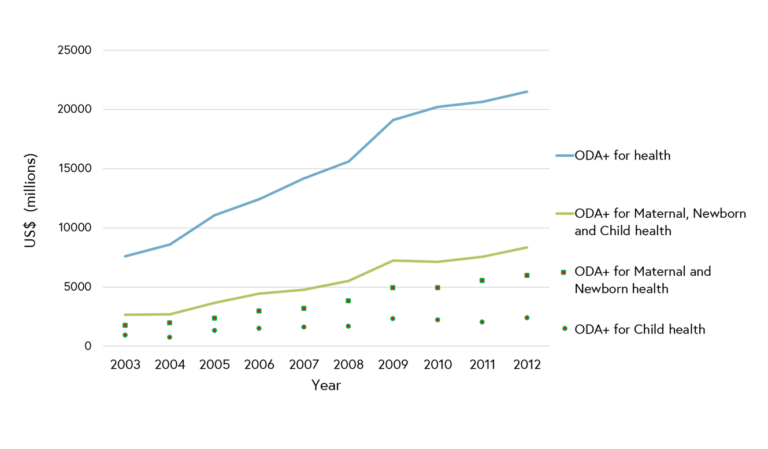 Figure 1. Official Development Assistance plus grants given by the Bill & Melinda Gates Foundation (ODA+) to maternal, newborn and child health worldwide, 2003-2012. (Arregoces et al., 2015)1
Figure 1. Official Development Assistance plus grants given by the Bill & Melinda Gates Foundation (ODA+) to maternal, newborn and child health worldwide, 2003-2012. (Arregoces et al., 2015)1
Between 2003 and 2013, ODA+ for all health investment increased from $7.6 billion to $24 billion (Figure 1). Proportionally, a small increase in allocation of spending to RMNCH was observed, with 35% of the total health spending by ODA+ in 2003 being compared to 39% in 2013. In absolute terms, this was from $3.8 billion to $13.0 billion, as follows:
- Reproductive and sexual health ODA increased from $1.4 billion to 4.4 billion
- Maternal/newborn health ODA increased from $0.8 billion to $2.3 billion
- Child health ODA from $1.6 billion to $6.3 billion 1
It is important to note that reproductive health funding is heavily dominated by HIV/AIDS earmarked funds. There has also been a surge in funding for family planning since 2011.
Child health received the greatest increase in ODA+ funding during this period (286%), followed by reproductive and sexual health (194%), and maternal and newborn health (164%) 2.
Does ODA+ go to the highest burden 75 Countdown countries?
The majority of ODA+ for reproductive, maternal, newborn and child health was spent in the 75 Countdown countries that suffer the highest mortality burden. Amongst these priority countries, funding increased annually by 14% from 2003 to 2013. In 2003, 88% of ODA+ spending on reproductive, maternal, newborn and child health (RMNCH) occurred in the 75 priority countries ($3.8 billion of the total $4.3 billion spent worldwide); compared to 93% in 2013 ($13.1 billion of the $14.0 billion spent worldwide) 1.
In 2011, ODA to maternal, newborn, and child health (MNCH) reduced for 60% of the 75 priority countries relative to 2010, with an increase in MNCH noted for only 40% of countries. Half of the countries that had a reduction in ODA to MNCH in 2011 had a further reduction in 2012. Of the 75 priority countries, Ethiopia received the largest level of ODA to MNCH in 2011 and Nigeria received the largest level in 2012. Turkmenistan received the lowest level of ODA to MNCH in both years. Mexico, China and Brazil, who are all middle-income countries, received the least ODA to child health per child and to MNH per livebirth in 2011 and 2012 2.
What do we know about spending on certain issues related to child health?
Just under 20% of funding to child health is for immunisation projects. While ODA mentioning newborns has increased from previous years (now at $1 billion, a 34-fold increase since 2003), this is most commonly alongside maternal and/or child health. The proportion of ODA noting interventions exclusively benefiting newborns, was only $6·0 million in 2012, representing 0·3% of ODA to maternal and newborn health. Whilst this is a 6·5-fold increase relative to 2003, the proportion remains very low given 45% of child deaths are now neonatal 2.
Improving the Health of Women, Children and Adolescents: from Evidence to Action


Improving the Health of Women, Children and Adolescents: from Evidence to Action
Reach your personal and professional goals
Unlock access to hundreds of expert online courses and degrees from top universities and educators to gain accredited qualifications and professional CV-building certificates.
Join over 18 million learners to launch, switch or build upon your career, all at your own pace, across a wide range of topic areas.




